Full Text (PDF)
Indian Journal of Forensic Medicine and Pathology 19(1):p 13-19, Jan - March 2026. | DOI: https://doi.org/10.21088/ijfmp.0974.3383.19126.2
Original Article
Safeguarding Patient Care: The Intersection of Documentation and Legal Aspects in Health Care
Debraj Banik, Ravindra S. Honnungar, Perumal P.3, Vinay S. Bannur
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Forensic Medicine and Pathology 19(1):p 13-19, Jan - March 2026. | DOI: https://doi.org/10.21088/ijfmp.0974.3383.19126.2
How Cite This Article:
Debraj B, Honnungar RS, Perumal P, et al. Bullets, Safeguarding Patient Care: The Intersection of Documentation and Legal Aspects in Health Care. Indian J Forensic Med Pathol. 2026;19(1):13-19.Timeline
Received : November 17, 2025
Accepted : January 03, 2026
Published : March 30, 2026
Abstract
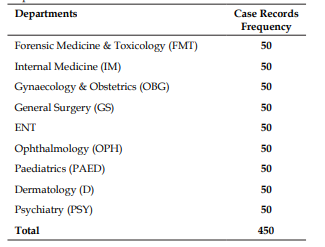
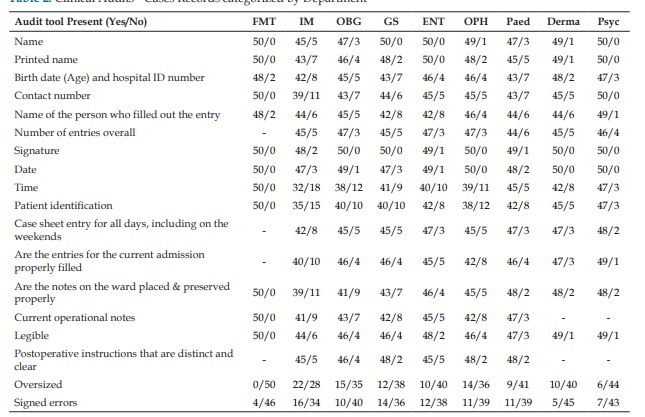
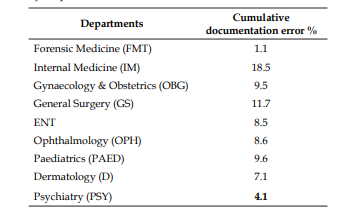
Introduction: Accurate, complete, and timely medical documentation is a cornerstone of safe and effective healthcare delivery. It ensures continuity of care, facilitates communication among healthcare providers, and serves as an essential medico-legal record. Inadequate or incomplete documentation can compromise patient safety, lead to diagnostic or therapeutic delays, and expose practitioners to legal liability. This study aims to assess the quality and completeness of inpatient medical records across multiple clinical departments in a tertiary care hospital and to examine the legal and ethical implications associated with documentation deficiencies. Materials and methods: A retrospective descriptive study was conducted in a 1250- bed multispecialty teaching hospital. Medical records from nine departments like Internal Medicine, Gynaecology & Obstetrics, Forensic Medicine & Toxicology, General Surgery, ENT, Ophthalmology, Paediatrics, Dermatology, and Psychiatry were evaluated. Using systematic random sampling, 50 inpatient case sheets were selected from each department, yielding a total sample of 450 records from April 2022 to April 2023. A structured 12-domain audit tool assessing demographics, admission details, history, examination findings, investigations, diagnosis, treatment notes, procedure-related entries, daily progress, discharge summaries, signatures, and supporting documents was used to analyze documentation completeness. Results: The audit revealed marked inter-departmental variation in documentation standards. Forensic Medicine & Toxicology demonstrated the highest accuracy, with only 1.1% cumulative documentation errors, reflecting stringent medico-legal protocols. The highest deficiencies were observed in Internal Medicine (18.5%) and General Surgery (11.7%), largely involving incomplete demographic entries, irregular clinical notes, missing time documentation, and inconsistent filing of supporting documents. Additional lapses were noted in operative notes, weekend entries, and signature authentication across several departments. Conclusion:Regular audits, training in medical record-keeping and implementation of standardized documentation protocols are essential to improve the quality of medical records and reduce medico-legal risks. Strengthening documentation practices supports better patient care, enhances institutional accountability, and safeguards healthcare professionals in legal contexts.
References
- 1. Chamisa I., Zulu B.M. Setting the records straight: A prospective audit of the quality of case notes in a surgical department. S Afr J Surg. 2007 Aug; 45(3): 92–95.
- 2. Foster S., Manser T. The effects of patient handoff characteristics on subsequent care: A systematic review and areas for future research. Acad Med. 2012; 87(8): 1105–24.
- 3. Kripalani S., LeFevre F., Phillips C.O., Williams M.V., Basaviah P., Baker D.W. Deficits in communication and information transfer between hospital-based and primary care physicians. JAMA. 2007; 297(8): 831–41.
- 4. Maegga B.T., Cox J., Malley K.D. Malaria in the southern highlands of Tanzania: a review of hospital records. Tanzan Health Res Bull 2005 Sep; 7(3): 125-32.
- 5. Mamlin B.W., Tierney W.M. The promise of information and communication technology in healthcare: extracting value from the chaos. Am J Med Sci. 2016; 351(1): 59–68.
- 6. World Health Organization, Regional Office for the Western Pacific. Medical Records Manual: A Guide for Developing Countries. Manila: WHO Regional Office for the Western Pacific; 2006. Available from: https://apps. who.int/iris/handle/10665/208125. Accessed 2025 Feb 19.
- 7. Häyrinen K., Saranto K., Nykänen P. Definition, structure, content, use and impacts of electronic health records: a review of the research literature. Int J Med Inform. 2008; 77(5): 291–304.
- 8. Menachemi N., Collum T.H. Benefits and drawbacks of electronic health record systems. Risk Manag Healthc Policy. 2011; 4: 47–55.
- 9. Feleke S.A., Mulatu M.A., Yesmaw Y.S. Medication administration error: magnitude and associated factors among nurses in Ethiopia. BMC Nurs. 2015; 14(1): 1–8.
- 10. Olivier J.M., Kyriacos U. Record keeping: selfreported attitudes, knowledge and practice behaviours of nurses in selected Cape Town hospitals: original research. Prof Nurs Today. 2011; 15(4): 8–9.
- 11. Ebrahimpour F., Pelarak F. Modified use of team-based learning to teach nursing documentation. Electron Physician. 2016; 8(1): 1764–70.
- 12. Ofi B., Sowunmi O. Nursing documentation: experience of the use of the nursing process model in selected hospitals in Ibadan, Oyo State, Nigeria. Int J Nurs Pract. 2012; 18(4): 354–62.
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects and therefore, does not require ethics approval.
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
Conflicts of Interest
No conflicts of interest in this work.
About this article
Cite this article
Debraj B, Honnungar RS, Perumal P, et al. Bullets, Safeguarding Patient Care: The Intersection of Documentation and Legal Aspects in Health Care. Indian J Forensic Med Pathol. 2026;19(1):13-19.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| November 17, 2025 | January 03, 2026 | March 30, 2026 |
DOI: https://doi.org/10.21088/ijfmp.0974.3383.19126.2
Keywords
Medical documentationLegal complianceConfidentialityEthicsHealthcare providersSearch for Similar Articles
Similar Articles
- Autopsy Study to Analyze Correlation between Survival Period & New Injury Severi...
- Neurocysticercosis as an Unrecognized Cause of Sudden Death: A CaseBased Study
- Analysis of Death Due to Pulmonary Embolism, a Case Series
- Suspected Adverse Event Following Immunization with Multisystem Inflammatory Res...
- Drone: A Smart Intelligent Framework Aiding Forensic Investigations
Article Level Metrics
Last UpdatedTuesday 28 July 2026, 05:56:50 (IST)
9858
Accesses
65
2464
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | November 17, 2025 |
| Accepted | January 03, 2026 |
| Published | March 30, 2026 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.