Full Text (PDF)
Indian Journal of Pathology: Research and Practice 15(1):p 85-90, Jan-Apr 2026. | DOI: 10.21088/ijprp.2278.148X.15126.10
Case Report
Placental Site Trophoblastic Tumor Originating in Tubal Ectopic Pregnancy: An Extremely Rare Case Report and Crucial Management Dilemma
Monish Gupta, Harshada Rajendra Bhangale
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Pathology: Research and Practice 15(1):p 85-90, Jan-Apr 2026. | DOI: 10.21088/ijprp.2278.148X.15126.10
How Cite This Article:
Bhangale HR, Gupta M. Placental Site Trophoblastic Tumor Originating in Tubal Ectopic Pregnancy: An Extremely Rare Case Report and Crucial Management Dilemma. Ind Jr of Path: Res and Practice. 2026;15(1):85-90.Timeline
Received : December 17, 2025
Accepted : January 20, 2026
Published : April 30, 2026
Abstract
Introduction: Placental Site Trophoblastic Tumor (PSTT) is a rare and distinct subtype of gestational trophoblastic neoplasia (GTN), arising from intermediate trophoblasts. Representing only 0.23% to 3% of GTD cases globally, PSTT is typically confined to the uterine implantation site.1 Ectopic localization of PSTT, particularly within the fallopian tube, is exceedingly rare, with approximately 20 cases reported in the published literature to date.3 This tumor presents a unique diagnostic challenge as its low production of human chorionic gonadotropin (betahCG) often contradicts standard diagnostic algorithms used for ectopic pregnancy, risking inappropriate conservative management.
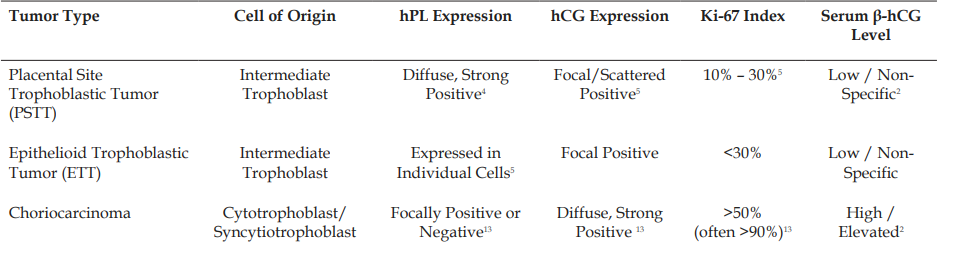
Case Presentation: A 32-year-old G2P1 patient presented with 6 weeks of amenorrhea, mild vaginal bleeding, and unilateral lower abdominal pain. Initial quantitative serum beta-hCG was 850 IU/L, with a suboptimal rise over 48 hours. Transvaginal ultrasound confirmed the absence of an intrauterine pregnancy (IUP) and identified a complex, highly vascularized mass (3.5 cm) in the right adnexa, necessitating laparoscopic right salpingectomy. Initial histopathology demonstrated an invasive trophoblastic proliferation. Definitive diagnosis of PSTT was established through immunohistochemistry (IHC), characterized by strong, diffuse positivity for Human Placental Lactogen (hPL), focal positivity for betahCG, and a low proliferative index (Ki-67: 15%)
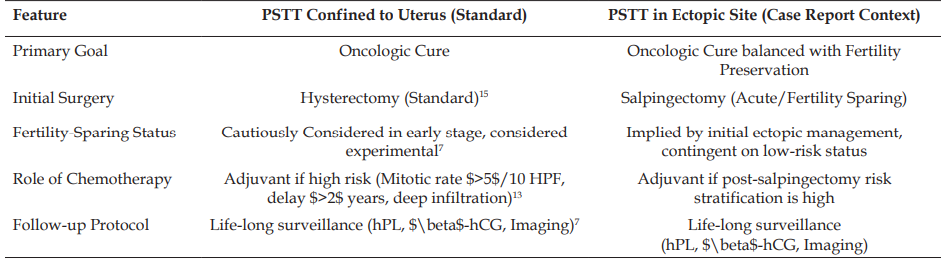
Management: The patient was staged as FIGO Stage I (localized disease). Given the localized nature and favorable prognostic factors (low mitotic rate, short interval since antecedent pregnancy), adjuvant chemotherapy was avoided. The patient was placed on a rigorous follow-up protocol involving long-term surveillance with periodic imaging (MRI) and monitoring of $\beta$-hCG and hPL, acknowledging the limitations of hCG monitoring alone for PSTT.
Conclusion: Ectopic PSTT is an ultra-rare malignancy whose clinical presentation is misleading due to low $\beta$-hCG production, challenging timely preoperative diagnosis.6 Definitive diagnosis hinges entirely on specialized pathological examination and IHC studies. While salpingectomy can be curative for localized, low-risk disease, specialized, long-term surveillance is mandatory to detect potential late recurrence, emphasizing the necessity of reporting such cases to inform international management guidelines.7
References
- 1. Yan S, Hu Y, Xi X. Placental site trophoblastic tumor: a case report and review of the literature. Front Surg. 2014;1:31.
- 2. Chang YL, Cheng HC, Chen YH, et al. Placental site trophoblastic tumor: a case report and review of the literature. Chang Gung Med J. 2005;28(11):801-5.
- 3. Shahib N, Onan MA, Karabulut AA, Guner H, Aral IB. Placental site trophoblastic tumor originating in a tubal ectopic pregnancy. Arch Gynecol Obstet. 2005;273(1):50-2.
- 4. Zhao J, Lyu J, Feng Z, et al. Diagnosis and treatment of placental site trophoblastic tumor. Int J Clin Exp Pathol. 2013;6(7):1448-51.
- 5. Al-Khabori T, Al-Salmani J, Al-Wahaibi S, et al. Placental site trophoblastic tumor (PSTT): a case report and review of the literature. J Med Case Rep. 2023;17(1):335.
- 6. Zheng Y, Li M, Jiao L. Placental site trophoblastic tumor: A case report and literature review. Oncol Lett. 2015;10(2):889-92.
- 7. Seckl MJ, Baas IO, Bolze PA, et al. Practical Guidelines for the Treatment of Gestational Trophoblastic Disease: Collaboration of the EOTTD-ESGO-GCIG-ISSTD. J Clin Oncol. 2024;42(29):3452-67.
- 8. Ngan HYS, Seckl MJ, Berkowitz RS, et al. Update on the diagnosis and management of gestational trophoblastic disease. Int J Gynaecol Obstet. 2018;143(Suppl 2):79-85.
- 9. Ali M, et al. Placental site trophoblastic tumor – a systematic review. Int J Acad Med Pharm. 2023;5(3):2178-82.
- 10. Soper JT. Gestational Trophoblastic Disease: Current Evaluation and Management. Obstet Gynecol. 2021;137(2):355-70.
- 11. Tenore JL. Ectopic pregnancy. Am Fam Physician. 2000;61(4):1080-8.
- 12. Barash JH, Buchanan EM, Hillson C. Ectopic Pregnancy: Diagnosis and Management. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2025 Oct 9].
- 13. Lu L, Shi X, Jiang Q, et al. A Review on the Pathogenesis and Clinical Management of Placental Site Trophoblastic Tumors. Front Oncol. 2019;9:937.
- 14. Feng Z, Zhao J, Lyu J, et al. Diagnosis and Management of Mixed Gestational Trophoblastic Neoplasia: A Study of 16 Cases and a Review of the Literature. Cancer Manag Res. 2019;11:10037-43.
- 15. Lurain JR. Gestational trophoblastic disease I: epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform mole. Am J Obstet Gynecol. 2010;203(6):531-9.
- 16. Bolze PA, Massardier J, Golfier F. Surgery including fertility-sparing treatment of GTD. Best Pract Res Clin Obstet Gynaecol. 2021;70:42-53.
- 17. Dr. Oracle. What is the percentage of conception after salpingectomy (tubal removal)? [Internet]. 2025 [cited 2025 Oct 9].
- 18. Perkumpulan Obstetri Dan Ginekologi Indonesia. Gestational Trophoblastic Neoplasia [Internet]. Jakarta: POI JAYA; 2021 [cited 2025 Oct 9].
- 19. Zhang X, et al. Comparing treatment strategies for placental site trophoblastic tumour (PSTT): study protocol for a systematic review and network meta-analysis. BMJ Open. 2024;14:e082574.
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
Whether all authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
Conflicts of Interest
The authors report no conflicts of interest in this work.
About this article
Cite this article
Bhangale HR, Gupta M. Placental Site Trophoblastic Tumor Originating in Tubal Ectopic Pregnancy: An Extremely Rare Case Report and Crucial Management Dilemma. Ind Jr of Path: Res and Practice. 2026;15(1):85-90.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| December 17, 2025 | January 20, 2026 | April 30, 2026 |
DOI: 10.21088/ijprp.2278.148X.15126.10
Keywords
Placental Site Trophoblastic TumorFallopian tubeRare malignancySearch for Similar Articles
Similar Articles
- Case Report of a Classic Case of Cervical SCC on Pap Smear
- Adenoid Cystic Carcinoma of the Vagina: A Case Report
- Revolutionizing Apheresis: The Transformative Impact of Artificial Intelligence...
- Evaluation of Biomarkers (Estrogen Receptor, Progesterone Receptor and HER-2) Im...
- Rectosigmoid Squamous Cell Carcinoma: A Rare Case Report
Article Level Metrics
Last UpdatedSunday 12 July 2026, 10:21:48 (IST)
2008
Accesses
11
434
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | December 17, 2025 |
| Accepted | January 20, 2026 |
| Published | April 30, 2026 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.