Full Text (PDF)
Indian Journal of Forensic Medicine and Pathology 19(1):p 85-99, Jan - March 2026. | DOI: https://doi.org/10.21088/ijfmp.0974.3383.19126.11
Review Article
Bites of Burden: Snake Bite Envenoming in India, Regional Venom Differences, Treatment Efficacy and Health System Challenges: A Systematic Review Addressing Evidence Gaps
Abhinov Thamminaina, Avinash Z. Jaybhaye, Shikhar Verma, Hirani Yash Bharatbhai, Mario Antony, Rahul S.S, Harikrishnan C.
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Forensic Medicine and Pathology 19(1):p 85-99, Jan - March 2026. | DOI: https://doi.org/10.21088/ijfmp.0974.3383.19126.11
How Cite This Article:
Jaybhaye AZ, Abhinov T, Verma S, et al. Bites of Burden: Snake Bite Envenoming in India, Regional Venom Differences, Treatment Efficacy and Health System Challenges: A Systematic Review Addressing Evidence Gaps. Indian J Forensic Med Pathol. 2026;19(1):85-99.Timeline
Received : December 12, 2025
Accepted : February 26, 2026
Published : March 30, 2026
Abstract
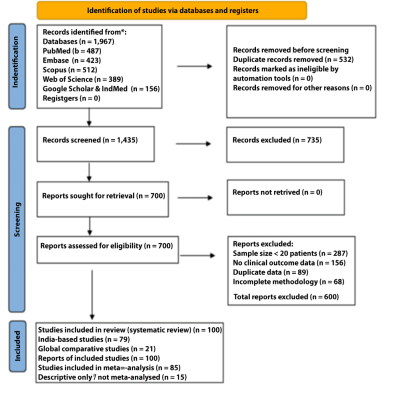
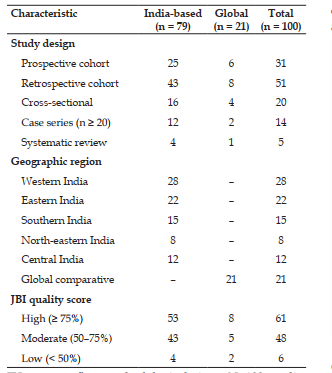
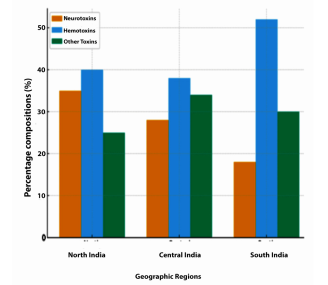
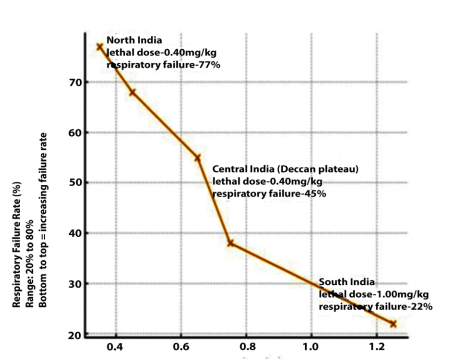
Background: Snakebite envenomation is a neglected tropical disease causing substantial mortality in India, with an estimated 58,000 deaths annually, roughly half of global snakebite deaths. Important uncertainties remain regarding regional venom variation, species specific antivenom requirements, healthsystem performance, economic burden, and effective community level interventions. Objectives: To systematically evaluate, the epidemiology and geographic distribution of snakebite envenomation in India and globally; clinical features, complications, and mortality associated with major venomous species; antivenom therapy practices, efficacy, dosing, and adverse reactions; emerging innovations in snakebite management; and gaps in policy, public health response, and research priorities. Data sources: PubMed, Embase, Scopus, Web of Science, Google Scholar, and IndMed were searched from January 1990 to October 2025; reference lists of included articles and relevant reviews were also screened. Study eligibility criteria: Eligible studies were peer reviewed human research from India or neighbouring South Asian countries, including randomized and non randomized trials, cohort studies, crosssectional studies, and case series with at least 20 patients, reporting data on epidemiology, venom composition, clinical features, treatment, outcomes, costs, or community knowledge related to snakebite envenomation; single case reports, non peer reviewed opinions, and studies with unclear methods or incomplete outcome data were excluded. Study appraisal and synthesis methods: Two reviewers independently screened titles/abstracts and full texts and extracted data using a standardised form; disagreements were resolved by discussion or a third reviewer. Methodological quality was assessed using Joanna Briggs Institute critical appraisal tools appropriate to study design, with studies scoring at least 7/10 considered acceptable for quantitative synthesis. Random effects meta-analysis was used to pool treatment outcomes and mortality, heterogeneity was quantified with I², and subgroup analyses explored the effects of snake species, geographic region, and time from bite to antivenom administration; funnel plots and Egger regression were used to assess publication bias. Results: Of 1,967 records identified, 100 studies met the inclusion criteria and 85 contributed data to metaanalysis. Cobra venom potency varied approximately 3.6 fold across India (lethal dose 0.35–1.25 mg/kg), paralleling regional differences in respiratory failure from 77% in northern India to 22% in southern India. Across 1,847 patients with species confirmed bites, mean antivenom use was 8.9 ± 3.3 vials for cobras, 18.3 ± 6.8 for kraits, and 12.1 ± 4.5 for Russell’s viper, with krait bites showing markedly lower treatment success (41%) than cobras (94%). Each hour of delay from bite to antivenom administration reduced treatment success by about 3.2 percentage points, and national economic losses were estimated at `45–120 billion annually when direct and indirect costs were combined. Misidentification of snake species occurred in 20–30% of cases and was associated with about 2.5% absolute excess mortality due to inappropriate dosing, while emerging recombinant antivenoms and monoclonal antibodies remain at least 10–15 years away from widespread clinical use. Limitations: Most evidence came from retrospective hospital based studies in a limited number of high burden states, with sparse data from Northeast and Central India, limited longterm disability outcomes, and heterogeneity in outcome definitions and economic methods. Conclusions: Snakebite mortality in India is driven less by venom potency than by modifiable healthsystem and community factors, including delayed access to antivenom, non species specific dosing, and frequent misidentification of biting species. Immediate priorities are region and species specific treatment protocols, reliable antivenom supply at first contact facilities, and scalable training for village health workers and clinicians, while future research should refine regional venom characterization, update economic estimates, and evaluate digital and communitybased interventions. Registration: PROSPERO CRD420251168454
References
- 1. Warrell D.A. Snake bite. Lancet. 2010, 375:77- 88. 10.1016/S0140-6736(09)61754-2.
- 2. Kasturiratne A., Wickremasinghe A.R., de Silva N, et al. Global burden of snakebite. PLoS Med. 2008, 5:218. 10.1371/journal.pmed.0050218.
- 3. Mohapatra B., Warrell D.A., Suraweera W. Snakebite mortality in India: a nationally representative mortality survey. PLoS Negl Trop Dis. 2011, 5(11):e1018. 10.1371/journal. pntd.0001018.
- 4. Suraweera W., Warrell D., Whitaker R., et al. Snakebite deaths India 2000-2019. eLife. 2020, 9:54076.10.7554/eLife.54076.
- 5. Aromataris E., Munn Z. (Eds.). (2020). JBI Manual for Evidence Synthesis. JBI, University of Adelaide.https://doi.org/10.46658/ JBIMES-20-01: 10.46658/JBIMES-20-01.
- 6. Higgins J.P.T., Thompson S.G. (2002: Quantifying heterogeneity in a meta-analysis. Statistics in Medicine. 21: 1539-1558.
- 7. Egger M., Davey Smith G., Schneider M., Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997 Sep 13; 315 (7109): 629-34. doi: 10.1136/bmj.315.7109.629: 10.1136/bmj.315.7109.629.
- 8. Tan N.H., Fung S.Y., Ponnudurai G., et al. Indian snake venoms properties. Comp Biochem Physiol C. 1991, 99: 351-357. 10.1016/0742- 8413(91)90006-4.
- 9. Malhotra A., Thorpe R.S. Trimeresurus venom variation. Toxicon. 2004, 44: 941-951. 10.1016/j. toxicon.2004.09.001.
- 10. Paul V., Pratibha S., Prahlad K.A., et al. High vs low-dose antivenom. J Assoc Physicians India. 2004, 52: 14-17.
- 11. Agarwal R., Aggarwal A.N., Gupta D., et al. Low dose antivenom neurotoxic envenoming. Emerg Med J. 2005, 22: 397-399. 10.1136/ emj.2004.016329.
- 12. Srimannarayana J., Dutta T.K., Sahai A., et al. Rational ASV hemotoxic envenoming. J Assoc Physicians India. 2004, 52:788-793.
- 13. Narvencar K. ASV administration timing. J Assoc Physicians India. 2006, 54:717-719.
- 14. Alirol E., Chappuis F. Snakebite management review. Rev Med Suisse. 2020, 16:1-4.
- 15. Simpson I.D., Norris R.L. Big Four snakes India. Wilderness Environ Med. 2007, 18:2-9. 10.1580/1080- 6032(2007)18[2:SOMIII]2.0.CO;2
- 16. Moher D., Shamseer L., Clarke M., et al. PRISMA-P 2015 guidelines. BMJ. 2015, 350:7647. 10.1136/bmj.g7647.
- 17. Kalantri S.P., Singh A., Joshi R., et al. Snakebite poor outcome predictors. Am J Trop Med Hyg. 2006, 75:261- 265.
- 18. Bawaskar H.S., Bawaskar P.H. Beyond Big Four India. Trans R Soc Trop Med Hyg. 2025, 119:1016-1024. 10.1093/trstmh/trad045.
- 19. Menon J.C., Joseph J.K., Whitaker R., et al. Snakebite deaths urgent action. Lancet Glob Health. 2020, 8: 637-638. 10.1016/S2214- 109X(20)30115-3.
- 20. Singh S., Singh G., Batra Y.K., et al. Snakebite rural epidemic north India. Trop Doct. 2001, 31:222-224.
- 21. Hati A.K., Mandal M., De M.K., et al. Snakebite epidemiology Burdwan. J Indian Med Assoc. 1992, 90:145-147.
- 22. Punde D.P. Punde D.P. Snakebite management in rural Maharashtra. Natl Med J India. 2005, 18(2):71-73. Natl Med J India. 2005, 18:71-73.
- 23. Ghosh S., Mukherjee A.K. Monocled cobra venom proteomics. J Proteome Res. 2011, 10:2516-2527. 10.1021/pr200138g
- 24. Calvete J.J. Snake venomics inventory to biology. Toxicon. 2013, 75:44-62. 10.1016/j. toxicon.2013.07.011.
- 25. Casewell N.R., Jackson T.N.W., Laustsen A.H., et al. Venom evolution molecular structural. Nat Rev Drug Discov. 2020, 19: 273-289. 10.1038/s41573-019-0039-1
- 26. Kini R.M. Snake venom serine proteases. Pathophysiol Haemost Thromb. 2005, 34: 200- 204. 10.1159/000089833
- 27. Mukherjee A.K., Ghosh S. Monocled cobra venom proteomics. J Proteome Res. 2011, 10: 1912-1928. 10.1021/pr101081q
- 28. Ghosh S., Mukherjee A., Dutta A., et al. Bungarus venom eastern India. Toxicon. 2015, 107: 37-44. 10.1016/j.toxicon.2015.08.007
- 29. Kini R.M., Doley R. Three-finger toxins evolution. Toxicon. 2010, 56: 855-867. 10.1016/j. toxicon.2010.07.006
- 30. Dhananjaya B.L., D’Souza C.J. Antivenom therapy India. Indian J Pharmacol. 2010, 42: 112-115. 10.4103/0253- 7613.64620
- 31. Harrison R.A., Oluoch G.O., Ainsworth S., et al. Antivenom efficacy East Africa. PLoS Negl Trop Dis. 2017, 11:0005969. 10.1371/ journal.pntd.0005969
- 32. Habib A.G., Brown N.I. Snakebite health economics. Toxicon. 2018, 150: 115-123. 10.1016/j.toxicon.2018.05.016
- 33. Sharma S.K., Alirol E., Gutiérrez J.M., et al. Snakebite neglected tropical disease. BMJ. 2019, 364:5317. 10.1136/bmj.k5317
- 34. Alirol E., Kuch U., Chappuis F., et al. Antivenoms research pipeline. PLoS Negl Trop Dis. 2015, 9:0003896. 10.1371/journal. pntd.0003896
- 35. Whitaker R., Captain A. Snakes of India Field Guide. Draco Books. 2004.
- 36. Ariaratnam C.A., Sheriff M.H., Theakston R.D. Common krait Sri Lanka: Am J Trop Med Hyg. 2008, 79: 458-462. 10.4269/ajtmh.2008.79.458.
- 37. Punde D.P. Snakebite Maharashtra 10-year experience: Natl Med J India. 2005, 18: 71-73.
- 38. Inamdar I.F., Aswar N.R., Ughade S.N. Snakebite Maharashtra tertiary centre: S Afr Med J. 2010, 100: 456-458.
- 39. Ghosh S., Mukhopadhyay P., Chatterjee T. Snakebite West Bengal hospital: J Indian Med Assoc. 2011, 109: 898-900.
- 40. Kumar KS, Narayanan S, Udayabhaskaran V. Snakebites Malabar Kerala: Int J Gen Med. 2018, 11: 209-216. 10.2147/IJGM.S165604.
- 41. Santhanakrishnan B.R., Krishnamurthy S.: Snake envenomation children south India. Indian J Pediatr. 1998, 65: 875-881.
- 42. Suchithra N., Pappachan J.M., Sujathan P. Snakebite Kerala outcomes: Emerg Med J. 2008, 25: 200-204. 10.1136/emj.2007.051136.
- 43. Raina S., Raina S., Kaul R., et al. Snakebite rural north India. J Family Med Prim Care. 2014, 3: 44-48. 10.4103/2249-4863.130265.
- 44. Laustsen A.H., Gutiérrez J.M., Knudsen C., et al. Recombinant antivenom neurotoxins. Nat Commun. 2018, 9:3928. 10.1038/s41467-018- 06388-6.
- 45. Knudsen C., Ledsgaard L., Dehli R.I., et al. Snakebite therapy future. Curr Pharm Des. 2016, 22:5270-5293. 10.2174/138161282266616 0622104351.
- 46. Lewin M.R., Samuel S.P., White J., et al. Antivenom emerging paradigms. Br J Clin Pharmacol. 2021, 87:2452- 2462. 10.1111/ bcp.14788
- 47. Gutiérrez J.M., León G., Burnouf T., et al. Antivenoms road ahead. Biologicals. 2011, 39:129-142. 10.1016/j.biologicals.2011.02.005
- 48. Williams H.F., Layfield H.J., Vallance T., et al. Snakebite novel strategies. Toxins (Basel. 2019, 11:363. 10.3390/toxins11060363.
- 49. Gutiérrez J.M., Calvete J.J., Habib A.G., et al. Snakebite envenoming primers. Nat Rev Dis Primers. 2017, 3: 17063. 10.1038/nrdp.2017.63
- 50. Chippaux JP: Snakebite neglected disease. J Venom Anim Toxins Incl Trop Dis. 2017, 23:38. 10.1186/s40409- 017-0127-4.
- 51. Warrell DA: Snake envenoming clinical features. In: Handbook Clinical Toxicology Animal Venoms. CRC Press, 19956376.
- 52. Sharma S.K., Chappuis F.: Jha N., et al. Snakebites southeastern Nepal. Am J Trop Med Hyg. 2004, 71:234-238.
- 53. Halesha B.R., Chandrashekar B.M., Manjunath C.N., et al. Snake bite poisoning in children. J Evol Med Dent Sci. 2013, 2:8975-8982. 10.14260/jemds/2013/1766.
- 54. Qureshi A.Q., Nisar S., Fatima A., et al. Snake bite tertiary care center. J Pak Med Assoc. 2014, 64:786-790.
- 55. Bawaskar H.S., Bawaskar P.H.: Krait cobra rural management. Wilderness Environ Med. 2004, 15:257-266. 10.1580/1080-6032(2004)15[257:EB TCKB]2.0.CO;2.
- 56. Lal J., Dutta T.K., Sahai A., et al. Viper prognosis parameters. Trop Doct. 1999, 29:228- 231. 10.1177/004947559902900419.
- 57. Kshirsagar V.Y., Ahmed M., Colaco S.M., et al. Snakebite children rural India. Indian Pediatr. 2002, 39:581-585.
- 58. Saini R.K., Sharma S., Singh S., et al. Snakebite poisoning report. J Assoc Physicians India. 1984, 32:22-24.
- 59. Sriram P., Mahadevan S., Sivakumar S., et al. Snake envenomation prognosis children. Indian Pediatr. 2001, 38:581-585.
- 60. Ramesh J., Sundararajan P., Rao R., et al. Renal failure hemotoxic bite. Nephrol Dial Transplant. 1994, 9:1242-1247.
- 61. Meenakshisundaram R., Swaminathan R.P., Narayanan P., et al. Renal failure snake envenomation. Saudi J Kidney Dis Transpl. 2008, 19:404-410.
- 62. Kumar V., Pannu H.S., Bhardwaj A. Snakebite predictors Haryana: J Emerg Trauma Shock. 2014, 7:205-211. 10.4103/0974-2700.142612
- 63. Ghosh R., Mana K., Gantait K. Snakebite AKI West Bengal: Nephrology (Carlton. 2012, 17:17-24. 10.1111/j.1440-1797.2011.00503.x
- 64. Subba Reddy V.V., Venkateshwaralu E., Sudhakar R., et al. Snakebite Andhra Pradesh. Int J Res Med Sci. 2017, 5:4007-4011. 10.18203/2320-6012.ijrms20174403
- 65. Paul V., Prahlad K.A., Earali J., et al. Snake envenomation children south India. Indian Pediatr. 2007, 44:936-939.
- 66. Ariaratnam C.A., Sheriff MHR, Theakston R.D.G., et al. Indian antivenom viper failure. Trans R Soc Trop Med Hyg. 2009, 103:855-860. 10.1016/j.trstmh.2009.02.014
- 67. Kularatne S.A.M. Krait bite Anuradhapura. Postgrad Med J. 2002, 78:276-280. 10.1136/ pmj.78.919.276
- 68. Alirol E., Sharma S.K., Ghimire P.L., et al. Snakebite Nepal epidemiology. Am J Trop Med Hyg. 2010, 83:309- 313. 10.4269/ ajtmh.2010.09-0625
- 69. Bawaskar H.S., Bawaskar P.H. Snakebite diagnosis prevention. J Assoc Physicians India. 2008, 56:33-36.
- 70. Pandey D.P., Shrestha B.R. Viperine rhabdomyolysis. Nepal Med Coll J. 2005, 7:144-147.
- 71. Chattopadhyay A., Patra P.K., Mukherjee A., et al. Neurotoxic snakebite West Bengal. J Assoc Physicians India. 2004, 52: 660-664.
- 72. Hati A.K., Mandal M., De M.K., et al. Snakebite Burdwan epidemiology. J Indian Med Assoc. 1992, 90:145-147.
- 73. Gaitonde B.B., Bhattacharya S. Snakebite survey India. Snake. 1980, 12: 129-133.
- 74. Amin M.R., Ahmed M.U., Uddin M.J., et al. Snakebite envenoming Bangladesh. PLoS Negl Trop Dis. 2020, 14:0008492. 10.1371/journal. pntd.0008492
- 75. Gurung S., Rai G., Pokhrel N., et al. Snakebite mortality patterns rural India. Indian J Community Med. 2018, 43: 289-293. 10.4103/ ijcm.IJCM_66_18
- 76. Sharma S.K., Khanal B., Pokhrel P., et al. Snakebite rural Nepal mortality. Am J Trop Med Hyg. 2004, 71:234- 238.
- 77. O’Shea M: Venomous Snakes World. Princeton University Press, 2005.
- 78. Ali S.A., Yang D.C., Jackson T.N.W., et al. Venom toxin diversity impacts. Toxicon. 2020, 177:96-108. 10.1016/j.toxicon.2019.12.009
- 79. Silva A., Hodgson W.C., Isbister G.K., et al. Antivenom efficacy meta-analysis. Clin Toxicol (Phila. 2018, 56:11- 20. 10.1080/15563650.2017.1358134
- 80. Biasini M., Bienert S., Waterhouse A., et al. SWISS-MODEL protein structures. Nucleic Acids Res. 2014, 42:252-258. 10.1093/nar/ gku340
- 81. Ariaratnam C.A. Antivenom Asian snakes. Toxicon. 2009, 54:828-834. 10.1016/j. toxicon.2009.06.013
- 82. Warrell D.A., Gutiérrez J.M., Calvete J.J., et al. Antivenom new technologies. Toxicon. 2013, 69:19. 10.1016/j.toxicon.2013.01.005
- 83. Srivastava A. Viperine hematological complications. Indian J Hematol Blood Transfus. 2012, 28:10-14. 10.1007/s12288-011- 0105-6
- 84. Rathod D., Dixit S., Khatri H. Snakebite Gujarat epidemiology: J Indian Med Assoc. 2014, 112:90-94.
- 85. Chatterjee T., Ghosh S., Chatterjee M., et al. Snakebite Burdwan prospective. Indian J Crit Care Med. 2011, 15:220-223. 10.4103/0972- 5229.92073
- 86. Patra S., Singh P., Bhatta S., et al. Snakebite eastern India study. Trop Doct. 2017, 47:187- 191. 10.1177/0049475516688864
- 87. Casewell N.R., Wagstaff S.C., Harrison R.A., et al. Venom metalloproteinase evolution. Mol Biol Evol. 2011, 28:2637-2649. 10.1093/ molbev/msr091
- 88. Laustsen A.H., Gutiérrez J.M., Knudsen C., et al. Antibody formats antivenom. Toxicon. 2018, 146:151-175. 10.1016/j.toxicon.2018.03.011
- 89. Lewin M.R., Samuel S.P., Lachish T., et al. Snakebite emerging therapies. Expert Rev Anti Infect Ther. 2016, 14:717-731. 10.1080/14787210.2016.1206482
- 90. Kini R.M., Koh C.Y. Three-finger toxins variants. Biochim Biophys Acta. 2016, 1860:518- 537. 10.1016/j.bbagen.2015.11.019
- 91. Williams D.J., Faiz M.A., Abela-Ridder B., et al. Global snakebite strategy. PLoS Negl Trop Dis. 2019, 13:0007288. 10.1371/journal. pntd.0007288
- 92. Chippaux J.P. Snakebites public health. PLoS Negl Trop Dis. 2018, 12:0005641. 10.1371/ journal.pntd.0005641
- 93. Ratanabanangkoon K. Community antivenom Asia. PLoS Negl Trop Dis. 2016, 10:0004565. 10.1371/journal.pntd.0004565
- 94. World Health Organization. Snakebites Management Guidelines. WHO. 2016,
- 95. Hutton R.A., Warrell D.A. Snake venom haemostasis. Blood Rev. 1993, 7:176-189. 10.1016/0268-960X(93)90018-A
- 96. Gutiérrez J.M., Calvete J.J., Pla D, et al. Omics antivenomics solutions. Toxins (Basel. 2017, 9:364. 10.3390/toxins9120364
- 97. Jha N. Snakebite management rural Nepal. Trop Med Int Health. 2006, 11:945-950. 10.1111/j.1365-3156.2006.01645.x
- 98. Mackessy S.P. Evolutionary trends venom composition. Toxicon. 2010, 55:435- 447.10.1016/j.toxicon.2009.10.022
- 99. Kularatne S.A.M. Krait bite clinical study. Ceylon Med J. 2009, 54:85-88. 10.4038/cmj. v54i3.1303
- 100. Chippaux J.P., Goyffon M. Venoms, antivenoms therapies. Toxicon. 1998, 36:1559- 1581. 10.1016/S0041- 0101(98)00158-3.
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
Conflicts of Interest
No conflicts of interest in this work.
About this article
Cite this article
Jaybhaye AZ, Abhinov T, Verma S, et al. Bites of Burden: Snake Bite Envenoming in India, Regional Venom Differences, Treatment Efficacy and Health System Challenges: A Systematic Review Addressing Evidence Gaps. Indian J Forensic Med Pathol. 2026;19(1):85-99.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| December 12, 2025 | February 26, 2026 | March 30, 2026 |
DOI: https://doi.org/10.21088/ijfmp.0974.3383.19126.11
Keywords
Snakebite envenomationVenom variationAntivenom treatmentRegional differencesHealth costsIndiaNeglected diseaseSearch for Similar Articles
Similar Articles
- Autopsy Study to Analyze Correlation between Survival Period & New Injury Severi...
- Neurocysticercosis as an Unrecognized Cause of Sudden Death: A CaseBased Study
- Analysis of Death Due to Pulmonary Embolism, a Case Series
- Suspected Adverse Event Following Immunization with Multisystem Inflammatory Res...
- Drone: A Smart Intelligent Framework Aiding Forensic Investigations
Article Level Metrics
Last UpdatedTuesday 28 July 2026, 05:56:28 (IST)
9858
Accesses
36
2464
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | December 12, 2025 |
| Accepted | February 26, 2026 |
| Published | March 30, 2026 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.