Full Text (PDF)
Indian Journal of Forensic Medicine and Pathology 11(3):p 192-201, Jul-Sep 2018. | DOI: 10.21088/ijfmp.0974.3383.11318.8
Original Article
Clinicopathologic Study of Granulomatous Lesions in the Bone Marrow
Sushma Belurkar, Anna Joseph Amprayil, Chethan Manohar
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator
Indian Journal of Forensic Medicine and Pathology 11(3):p 192-201, Jul-Sep 2018. | DOI: 10.21088/ijfmp.0974.3383.11318.8
How Cite This Article:
Timeline
Received : July 16, 2018
Accepted : August 09, 2018
Published : September 30, 2018
Abstract
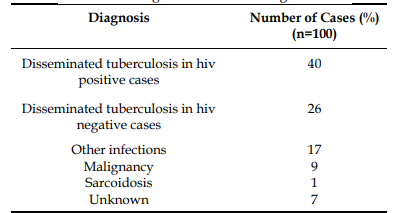
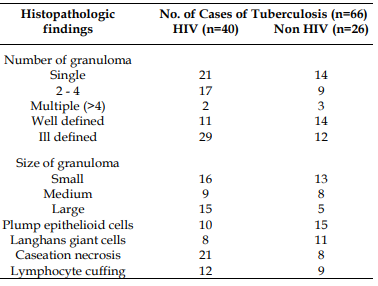
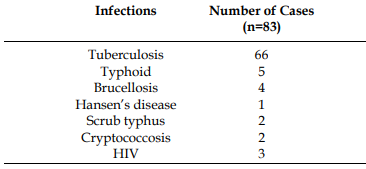
Introduction: Granulomatous lesion in the bone marrowis not a common finding and can be attributed to a variety of conditions ranging from infections to malignancies to drugs. Though tuberculosis is the most common etiology, bone marrow granulomas can be associated with a number of infections and other non infective conditions. The incidence of bone marrow granulomas has been increasing over the years due to the increasing surge of HIV infection. Aims: This study basically aims to study the prevalence of bone marrow granulomas, to identify the various causes and to study the pattern of granulomas in different conditions. Materials & Methods: This is a retrospective analysis of 100 cases of bone marrow granulomas conducted in the Clinical Laboratory of Kasturba hospital for a period of four and a half years from January 2009 to May 2013.The clinical details were collected from medical records and bone marrow biopsy slides were retrieved and studied. Results: Out of the 100 cases, 66% cases were diagnosed as tuberculosis. 17% cases were due to other infections like Typhoid fever (5%), Brucellosis (4%), Scrub typhus (2%), Hansen’s disease (1%), Cryptococcosis (2%) and HIV infection itself without any other opportunistic infections (3%). Malignancies accounted for 9% cases, Sarcoidosis (1%) and in 7% cases a definitive diagnosis was not reached. Among the 66 cases of tuberculosis, 40 (60%) cases were immunodeficient due to HIV infection. HIV positive cases predominantly showed single (52%), ill defined granulomas (73%), with caseation necrosis (52%), while HIV negative cases predominantly showed single (54%), small (50%), well defined or ill defined granulomas with plump epithelioid cells (58%) and Langhans giant cells (42%). Conclusion: There can be varied etiology for bone marrow granulomas with tuberculosis being the most common cause.The morphology and pattern of granulomas can aid in the diagnosis of the condition hence study of bone marrow for granulomas should be considered as an important diagnostic tool in such conditions.
References
- 1. Kumar V, Abbas AK, Fausto N, Aster JC, editors. Acute and chronic inflammation. In: Robbins and Cotran pathologic basis of disease. 8th ed. Philadelphia: Elsevier Saunders; 2010. p. 70-4.
- 2. Bodem CR, Hamory BH, Taylor HM, Kleopfer L. Granulomatous bone marrow disease: a review of the literature and clinicopathologic analysis of 58 cases. Medicine (Baltimore). 1983;62(6):372-83.
- 3. Vilalta-Castel E, Valdes-Sanchez MD, Guerra-Vales JM, et al. Significance of granulomas in bone marrow: a study of 40 cases. Eur J Haematol. 1988;41(1):12-6.
- 4. Basu D, Saravana R, Purushotham B, Ghotekar LH. Granulomas in bone marrow: a study of fourteen cases. Indian J Pathol Microbiol. 2005;48(1):13-6.
- 5. Brackers de Hugo L, et al. Granulomatous lesions in bone marrow: clinicopathologic findings and significance in a study of 48 cases. Eur J Intern Med. 2013;24(5):468-73.
- 6. Peace G. Granulomatous lesions in the bone marrow. Blood. 1956;11(8):720-34.
- 7. Eid A, Carion W, Nystrom JS. Differential diagnoses of bone marrow granuloma. West J Med. 1996;164(6):510-5.
- 8. Nichols L, Florentine B, Lewis W, Sattler F, Rarick MU, Brynes RK. Bone marrow examination for the diagnosis of mycobacterial and fungal infections in the acquired immunodeficiency syndrome. Arch Pathol Lab Med. 1991;115:1125-32.
- 9. Castella A, et al. The bone marrow in AIDS: a histologic, hematologic and microbiologic study. Am J Clin Pathol. 1985;84(4):425-32.
- 10. Shin SM, Paik IK, Cho HI. Bone marrow pathology of culture proven typhoid fever. J Korean Med Sci. 1994;9(1):57-63.
- 11. Chung HJ, Chi HS, Cho YU, et al. Bone marrow fibrin-ring granuloma: review of 24 cases. Korean J Lab Med. 2007;27(3):182-7.
- 12. Rywlin AM. Histopathology of the bone marrow. Boston: Little, Brown & Co; 1976. p. 170.
- 13. Suster S, et al. Non-granulomatous involvement of bone marrow in lepromatous leprosy. Am J Clin Pathol. 1989;92(6):797-801.
- 14. O’Carroll DI, McKenna RW, Brunning RD. Bone marrow manifestations of Hodgkin disease. Cancer. 1976;38(4):1717-28.
- 15. Sacks EL, Donaldson SS, Gordon J, Dorfman RF. Epithelioid granulomas associated with Hodgkin disease: clinical correlations in 55 previously untreated patients. Cancer. 1978;41(2):562-7.
- 16. Abrams J, Pearl P, Moody M, Schimpff SC. Epithelioid granuloma revisited: long-term follow-up in Hodgkin disease. Am J Clin Oncol. 1988;11(4):456-60.
- 17. Yanardag H, Pamuk GE, Karayel T, Demirci S. Bone marrow involvement in sarcoidosis: an analysis of 50 bone marrow samples. Haematologia. 2002;32(4):419-25.
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
Whether all authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
Conflicts of Interest
The authors report no conflicts of interest in this work.
About this article
Cite this article
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator
| Received | Accepted | Published |
|---|---|---|
| July 16, 2018 | August 09, 2018 | September 30, 2018 |
DOI: 10.21088/ijfmp.0974.3383.11318.8
Keywords
Bone MarrowGranulomaTuberculosisHIVDrugsMorphologySearch for Similar Articles
Similar Articles
- Pesticide Contamination in Indian Agricultural and Residential Areas: A Compara...
- Forensic Age Estimation using CBCT-Derived Mandibular Morphometrics: A Comparat...
- A 2 Years Retrospective Study of the Spectrum of Poisoning in a Tertiary Care C...
- Knowledge and Attitude of MBBS Students Regarding Post Mortem Examination: A Cr...
- Sudden Death in a 7-year-old Child Due to Neoplasm: A Case Report
Article Level Metrics
Last UpdatedWednesday 08 July 2026, 06:33:19 (IST)
7722
Accesses
2
2137
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | July 16, 2018 |
| Accepted | August 09, 2018 |
| Published | September 30, 2018 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator