Full Text (PDF)
Indian Journal of Obstetrics and Gynecology 12(3):p 111-116, July-September 2024. | DOI: http://dx.doi.org/10.21088/ijog.2321.1636.12324.1
Original Article
Analysis of Risk Factors Causing still Births in a Tertiary Care Hospital of Northern India
Seema Singhal, Rajesh Kumari, Divya Wadhawan, Pratima Mittal
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Obstetrics and Gynecology 12(3):p 111-116, July-September 2024. | DOI: http://dx.doi.org/10.21088/ijog.2321.1636.12324.1
How Cite This Article:
Singhal S, Kumari R, Wadhawan D, et al. Analysis of risk factors causing still births in a tertiary care hospital of northern India. Indian J Obstet Gynecol. 2024;12(3):111-6.Timeline
Received : April 02, 2024
Accepted : June 05, 2024
Published : June 29, 2024
Abstract
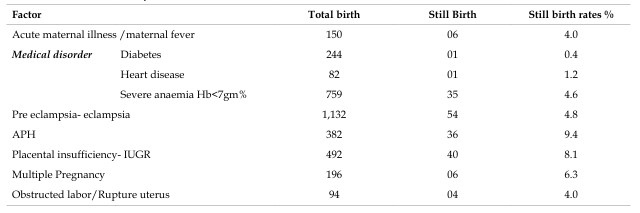
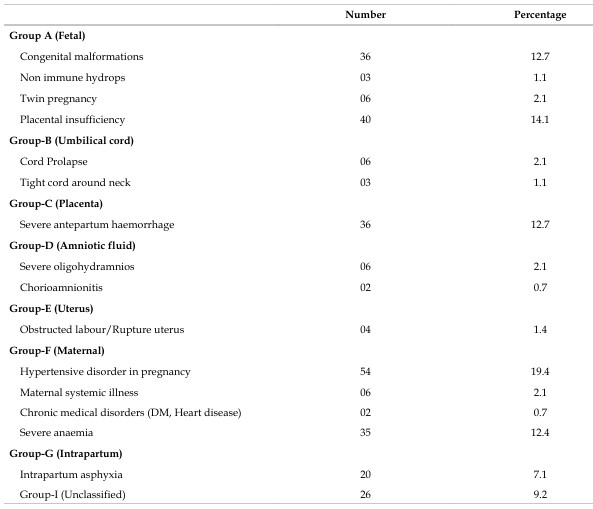
Background: In developing countries most deliveries take place at home or peripheral settings, therefore, information on causes of still birth remain insufficient. ReCoDe (Relevant condition at death) is a classification system that helps to understand causes of still births in low resource settings. Aims: Present study was conducted to identify various clinical conditions that could lead to still births and to classify the still births according to Re.Co.De system. Materials and Methods: An observational study was conducted for six months and records of all the deliveries including still births were reviewed. The causes were classified according to the ReCoDe classification. Any association between maternal factors and still births was analysed. Results: During study period 11,748 births occurred and 283 of them were still births. Still birth rate was 2.41% (24.1/1000 births). 9.5% (27) of still births were intrapartum and 90.5% (256) were ante partum. 9.4% of still births occurred in women having antepartum haemorrhage and 8.1% with fetalgrowth restriction. This was followed by multiple pregnancy, hypertensive disorders of pregnancy and obstructed labour. When classified as per ReCoDe cause of still birth could not be explained in 9.4% cases.
References
- 1. Cousens S, Blencowe H, Stanton C, et al. National, regional, and worldwide estimates of stillbirth rates in 2009 with trends since 1995: a systematic analysis. Lancet 2011; 377:13191330.
- 2. Lawn JE, Blencowe H, Pattinson R, et al., for The Lancet’s Stillbirths Series steering committee. Stillbirths: where? When? Why? How to make the data count? Lancet 2011; 377:1448–1463.
- 3. Singh Abha, Toppo A. Re.Co.De.: A Better Classification for Determination of Still Births. The Journal of Obstetrics and Gynecology of India 2011; 61(6):656–658.
- 4. Flenady V, Froen JF, Pinar H, Torabi R, Saastad E, Guyon G, et al. An evaluation of classification systems for stillbirth. BMC Pregnancy Childbirth. 2009;9:24.
- 5. Gardosi J, Kady SM, McGeown P, Francis A, Tonks A.Classification of stillbirth by relevant condition at death (Re.Co.De): population based cohort study. Br Med J. 2005;331:1113–17.
- 6. Reddy U, Ko C-W, Willinger M. Maternal age and the risk of stillbirth throughout pregnancy in the United States. AJOG. 2006;195:764–70.
- 7. Baquil AH, Choil Y, Williams EK, Arifeen SE, Mannan I, Darmstadt GL et al. Levels, timing, and etiology of stillbirths in Sylhet district of Bangladesh. BMC Pregnancy and Childbirth 2011; 11:25 http://www.biomedcentral. com/1471-2393/11/25
- 8. Sahu M, Agarwal A, Das V, et al. Advanced maternal age and obstetric outcome. J Obstet Gynecol India. 2007;57:320–3.
- 9. Elizabeth G. Raymond,Sven Cnattingius, John L. Kiely. Effects of maternal age, parity, and smoking on the risk of stillbirth. BJOG.1994;101(4) :301–6.
- 10. Savvas E, Evangelos A. Case control study of factors associated with intrauterine fetal deaths. Med Gen Med. 2004;6:53.
- 11. The Stillbirth Collaborative Research Network Writing Group. Causes of death among stillbirths. JAMA 2011; 306:2459–2468.
- 12. M. Jones DW, Weiss HA, Changalucha J, et al. Adverse birth outcomes in United Republic of Tanzania impact and prevention of maternal risk factors. Bull World Health Organ. 2007;85:9–18.
- 13. J. Wapner RJ, Lewis D. Genetics and metabolic causes of stillbirths. Semin Perinatol. 2002;26:70–4.
- 14. Korteweg FJ, Gordijn SJ, Timmer A, Holm JP, Ravise JM, Erwich JJ. A placental cause of intra uterine fetal death depends on the perinatal mortality classification system used. Placenta. 2008;29:71–80.
- 15. CESDI - Confidental enquiry into Stillbirths and Deaths in infancy. 8th Annual Report. 2001.
- 16. Helgad_ottir LB, Turowski G, Skjeldestad FE, Jacobsen AF, Sandset PM, Roald B, Jacobsen E-M. Classification of stillbirths and risk factors by cause of death – a case-control study. Acta Obstet Gynecol Scand 2013; 92:325–333.
- 17. Serena C, Marchetti G, Rambaldi MP, Ottanelli S, Tommaso MD, Avagliano L, Pieralli A, Mello G, Mecacci F. Still birth and fetal growth restriction. Journal of Maternal-Fetal and Neonatal Medicine 2013; 26:1, 16-20.
Data Sharing Statement
There are no additional data available.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval
Acknowledgements
Information Not Provided
Conflicts of Interest
No conflicts of interest in this work.
About this article
Cite this article
Singhal S, Kumari R, Wadhawan D, et al. Analysis of risk factors causing still births in a tertiary care hospital of northern India. Indian J Obstet Gynecol. 2024;12(3):111-6.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| April 02, 2024 | June 05, 2024 | June 29, 2024 |
DOI: http://dx.doi.org/10.21088/ijog.2321.1636.12324.1
Keywords
Still birthRe.Co.De classificationPerinatal auditRisk factorsSearch for Similar Articles
Similar Articles
- When Eclampsia Strikes the Brain Twice
- Emergency Management of Cesarean Scar Pregnancy: A Rare Case of Life-Threatenin...
- The Efficacy of Structured Teaching Programs in Enhancing Pregnancy Management...
- Audit of Caesarean Sections by the Robson Ten Group Classification: A Six-Month...
- A Cross-Sectional Study on the Epidemiology and Risk Factors of Uterine Fibroids
Article Level Metrics
Last UpdatedThursday 18 June 2026, 04:27:33 (IST)
1422
Accesses
2
152
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | April 02, 2024 |
| Accepted | June 05, 2024 |
| Published | June 29, 2024 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.