Full Text (PDF)
Indian Journal of Anesthesia and Analgesia 11(2):p 87-94, April - June 2024. | DOI: https://doi.org/10.21088/ijaa.2349.8471.11124.6
Case Report
Detect it Early! Fat Embolism Syndrome (FES)
Ashish Nair, Athira CN, Prashant P Jedge
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Anesthesia and Analgesia 11(2):p 87-94, April - June 2024. | DOI: https://doi.org/10.21088/ijaa.2349.8471.11124.6
How Cite This Article:
Nair A, Athira CN, Jedge PP. Detect it early! Fat embolism syndrome (FES). Ind J Anesth Analg. 2024;11(2):87-94.Timeline
Received : January 09, 2024
Accepted : February 20, 2024
Published : June 29, 2024
Abstract
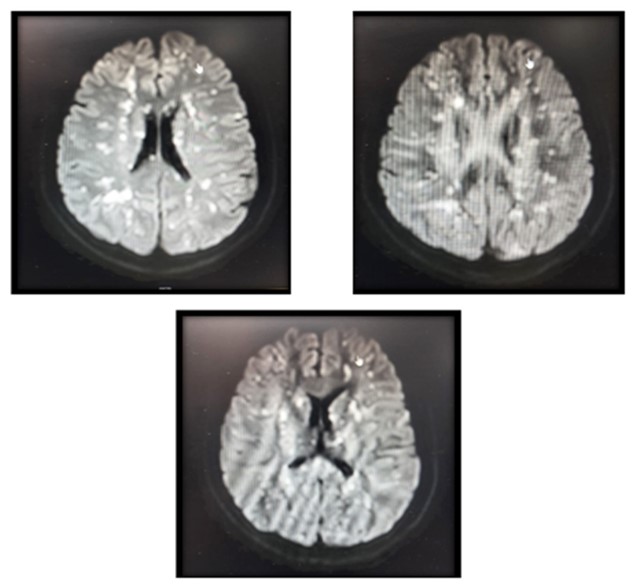
Fat embolism syndrome (FES) is a rare but a serious clinical catastrophe occurring after traumatic injury to long bones. Cerebral involvement in the absence of pulmonary or dermatological manifestation on initial presentation may delay the diagnosis of cerebral fat embolism (CFE). Cerebral fat embolism typically occurs in patients with bony fractures (usually long bones of the lower limb). Fat embolism syndrome has an incidence of 1-3% following long bone fractures and 33% in patients with bilateral long bone fractures. We discuss a case series of CFE which posed a challenge in diagnosis. The clinical presentations of these patients did not satisfy the commonly used clinical criteria for aiding the diagnosis of FES. Early MRI brain (DWI and T2 weighted sequences) in patients with neurological symptoms after trauma even in the absence of pulmonary and dermatological findings should be the goal.
References
- 1. Luff D, Hewson DW. Fat embolism syndrome. BJA Educ. 2021;21(9):322–8.
- 2. Kainoh T, Iriyama H, Komori A, Saitoh D, Naito T, Abe T. Risk Factors of Fat Embolism Syndrome After Trauma: A Nested Case-Control Study With the Use of a Nationwide Trauma Registry in Japan. Chest 2021;159(3):1064–71.
- 3. Lempert M, Halvachizadeh S, Ellanti P, et al. Incidence of fat embolism syndrome in femur fractures and its associated risk factors over time—A systematic review. J Clin Med. 2021;10(12).
- 4. Gosling HR, Pellegrini VD. Fat Embolism Syndrome A Review of the Pathophysiology and Physiological Basis of Treatment [Internet]. Available from: http://journals.lww.com/clinorthop.
- 5. Kosova E, Bergmark B, Piazza G. Fat embolism syndrome. Circulation 2015;131(3):317–20.
- 6. Scarpino M, Lanzo G, Lolli F, Grippo A. From the diagnosis to the therapeutic management: Cerebral fat embolism, a clinical challenge. Int J Gen Med 2019;12:39–48.
- 7. Tsai IT, Hsu CJ, Chen YH, Fong YC, Hsu HC, Tsai CH. Fat embolism syndrome in long bone fractureclinical experience in a tertiary referral center in Taiwan. Journal of the Chinese Medical Association 2010;73(8):407–10.
- 8. Vetrugno L, Bignami E, Deana C, et al. Cerebral fat embolism after traumatic bone fractures: a structured literature review and analysis of published case reports. Scand J Trauma Resusc Emerg Med. 2021;29(1).
- 9. baker1971.
- 10. Parizel PM, Demey; H E, Veeckmans; G, et al. Early Diagnosis of Cerebral Fat Embolism Syndrome by Diffusion-Weighted MRI (Starfield Pattern) [Internet]. 2001. Available from: http:// ahajournals.orgErdem E, Namer IJ, Saribas O, et al. Cerebral fat embolism studied with MRI and SPECT. 1993.
- 11. He Z, Shi Z, Li C, et al. Single-case metanalysis of fat embolism syndrome. Int J Cardiol 2021;345:111–7.
- 12. Schonfeld SA, Ploysongsang R, Dilisio JD, et al. Fat Embolism Prophylaxis with Corticosteroids A Prospective Study in High-Risk Patients [Internet]. 1983. Available from: http://annals.org/pdfaccess. ashx?url=/data/journals/aim/19602/.
- 13. Pinney’ SJ, Keating2 JF, Meek’ RN. Fat embolism syndrome in isolated femoral fractures: does timing of nailing influence incidence? 1998.
- 14. Baig M, Curtin W. A Simple and Easy Intramedullary Lavage Method to Prevent Embolism During and After Reamed Long Bone Nailing. Cureus 2017.
- 15. Mellor A, Soni N.Fat embolism.Anesthesia. 2001; 56:145–154.
- 16. Pell AC, Hughes D, Keating J, Christie J, Busuttil A, Sutherland GR.Brief report: fulminating fat embolism syndrome caused by paradoxical embolism through a patent foramen ovale.N Engl J Med. 1993; 329:926–929. doi: 10.1056/NEJM199309233291305.
- 17. Gupta A, Reilly CS.Fat embolism. Continuing Education in Anaesthesia, Critical Care & Pain. 2007; 7:148–151.
- 18. Bulger EM, Smith DG, Maier RV, Jurkovich GJ.Fat embolism syndrome. A 10-year review. Arch Surg. 1997; 132:435–439.
- 19. Forteza AM, Koch S, Romano JG, Zych G, Bustillo IC, Duncan RC, et al. Transcranial doppler detection of fat emboli.Stroke. 1999; 30:2687–2691. doi: 10.1161/01. STR.30.12.2687.
- 20. Takahashi M, Suzuki R, Osakabe Y, Asai JI, Miyo T, Nagashima G, et al. Magnetic resonance imaging findings in cerebral fat embolism: correlation with clinical manifestations.J Trauma. 1999; 46:324–327.
- 21. Suh SI, Seol HY, Seo WK, Koh SB.Cerebral fat embolism: susceptibility-weighted magnetic resonance imaging.Arch Neurol. 2009; 66:1170. doi: 10.1001/ archneurol.2009.173.
- 22. Kamenar E, Burger PC.Cerebral fat embolism: a neuropathological study of a microembolic state.Stroke. 1980; 11:477–484. doi: 10.1161/01.STR.11.5.477.
- 23. Lindeque B, Schoeman H, Dommisse G, Boeyens MC, Vlok AL. Fat embolism and the fat embolism syndrome. J Bone Joint Surg 1987;69B: 128-31.
- 24. Schonfeld SA, Ploysongsang Y, DiLisio R, Crissman JD, Miller E, Hammerschmidt DE, et al. Fat embolism prophylaxis with corticosteroids. A prospective study in high-risk patients. Ann Intern Med 1983;99:438-43.
Data Sharing Statement
There are no additional data available.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
Information not provided.
Conflicts of Interest
The authors report no conflicts of interest in this work.
About this article
Cite this article
Nair A, Athira CN, Jedge PP. Detect it early! Fat embolism syndrome (FES). Ind J Anesth Analg. 2024;11(2):87-94.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| January 09, 2024 | February 20, 2024 | June 29, 2024 |
DOI: https://doi.org/10.21088/ijaa.2349.8471.11124.6
Keywords
Cerebral fat embolismFat embolism syndromeMagnetic resonance imagingSearch for Similar Articles
Similar Articles
- Awake Fibreoptic Intubation for Airway Management in Massive Thyroid Enlargement...
- A Case of Thoracotomy with One Lung Ventilation for Carcinoma Oesophagus
- A Case of Empyema for Thoracotomy and Decortication-Anaesthesia Management
- Full Mouth Rehabilitation in a 3-Year-Old Female Child with Repaired Tetralogy o...
- Do Gel Manicures Affect SpO2 Readings ? A Clinical Investigation
Article Level Metrics
Last UpdatedTuesday 14 July 2026, 09:01:18 (IST)
5690
Accesses
11
679
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | January 09, 2024 |
| Accepted | February 20, 2024 |
| Published | June 29, 2024 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.