Full Text (PDF)
Indian Journal of Anesthesia and Analgesia 13(2):p 106-110, April-June 2026. | DOI: https://doi.org/10.21088/ijaa.2349.8471.13226.10
Case Report
Awake Fibreoptic Intubation for Airway Management in Massive Thyroid Enlargement: A Case Report
Rajesh Kumar, Sanjay Kumar, Rekha Kumari, Sunil Kumar, Radheshyam null, Anurag Kumar, Majid Anwer
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license
enables reusers to distribute, remix, adapt, and build upon the material in any
medium or format for noncommercial purposes only, and only so long as
attribution is given to the creator.
Indian Journal of Anesthesia and Analgesia 13(2):p 106-110, April-June 2026. | DOI: https://doi.org/10.21088/ijaa.2349.8471.13226.10
How Cite This Article:
Sanjay Kumar, Rekha Kumari, Rajesh Kumar, et al. Awake Fibreoptic Intubation for Airway Management in Massive Thyroid Enlargement: A Case Report. Ind J Anesth Analg. 2026; 13(2): 106-110.Timeline
Received : March 03, 2026
Accepted : April 07, 2026
Published : June 30, 2026
Abstract
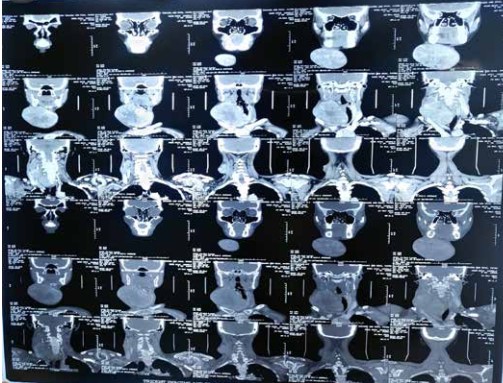
Massive thyroid enlargement can significantly distort upper airway anatomy by causing tracheal compression, lateral deviation, and restricted neck mobility, thereby increasing the risk of difficult mask ventilation and tracheal intubation. Induction of general anaesthesia before securing the airway in such patients may precipitate airway collapse and catastrophic hypoxia. We report the case of a 55-year-old female presenting with a progressively enlarging anterior neck swelling and mild dyspnoea, with clinical features suggestive of an anticipated difficult airway. Preoperative assessment revealed distorted airway anatomy, limited neck extension, and possible tracheal compression. A planned strategy of awake fibreoptic intubation (FOI) was adopted following comprehensive airway topicalisation using lignocaine nebulisation and targeted superior laryngeal and transtracheal nerve blocks. Awake oral fibreoptic intubation was successfully performed while preserving spontaneous ventilation. General anaesthesia was subsequently induced, and thyroid surgery proceeded uneventfully. The patient was extubated after full recovery and monitored postoperatively without airway complications. This case highlights the importance of meticulous airway assessment. It demonstrates awake fibreoptic intubation as a safe and reliable technique in patients with massive thyroid enlargement and an anticipated difficult airway.
References
- 1. Ran G., Ning M., Zhang X. Awake fiberoptic intubation in a patient with a large thyroid tumor invading the trachea: a case report. Am J Transl Res. 2022; 14: 2497–2500.
- 2. Patil V.H., Huddar K.S., Barsagade W.S., Rao A.U. Airway management of huge thyroid swelling having tracheal deviation: challenges faced. Indian J Clin Anaesth. 2022; 9: 514–517.
- 3. Ladha G.G., Patel N.D., Kavishvar N. Airway management of a huge thyroid swelling with retrosternal extension by awake intubation using loco-sedative technique. J Anaesthesiol Clin Pharmacol. 2015; 31: 272–274. doi:10.4103/0970-9185.155160
- 4. Abdelmalak B.B., Makary L., Hoban J.D., et al. Dexmedetomidine versus propofol sedation during awake fiberoptic intubation: randomized controlled trial. Anesth Analg. 2019; 129: 154–161. doi:10.1213/ANE.0000000000003733
- 5. Mondal S., Ghosh S., Bhattacharya S., et al. Comparison of dexmedetomidine and remifentanil for awake fiberoptic intubation: randomized controlled trial. J Clin Anesth. 2015; 27: 483–489. doi:10.1016/j.jclinane.2015.04.005
- 6. Hu R., Liu J.X., Jiang H. Dexmedetomidine versus midazolam for sedation during awake fiberoptic nasotracheal intubation: randomized controlled trial. J Clin Anesth. 2013; 25: 211–217. doi:10.1016/j.jclinane.2012.08.009
- 7. Apfelbaum J.L., Hagberg C.A., Connis R.T., Abdelmalak B.B., Agarkar M., Dutton R.P., et al.2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology. 2022; 136(1): 31–81. doi:10.1097/ALN.0000000000004002
- 8. Frerk C., Mitchell V.S., McNarry A.F., Mendonca C., Bhagrath R., Patel A., et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. Br J Anaesth. 2015; 115(6): 827–848. doi:10.1093/bja/aev371
- 9. Ovassapian A., Tuncbilek M., Weitzel E.K., Joshi C.W. Airway management in adult patients with deep neck infections: a case series and review. Anesth Analg. 2005; 100(2): 585–589. doi:10.1213/01.ANE.0000141526.32741.65
- 10. Rosenblatt W.H., Sukhupragarn W. Airway management in thyroid surgery. Otolaryngol Clin North Am. 2010; 43(2): 251–265. doi:10.1016/j.otc.2010.01.004
- 11. Amathieu R., Sauvat S., Reynaud P., Slavov V., Luis D., Dinca A, et al. Difficult intubation in thyroid surgery: myth or reality? Anesth Analg. 2006; 103(4): 965–968. doi:10.1213/01.ane.0000237275.49948.3c
- 12. Law J.A., Broemling N., Cooper R.M., Drolet P., Duggan L.V., Griesdale D.E., et al. The difficult airway with recommendations for management—Part 1: difficult tracheal intubation. Can J Anaesth. 2013; 60(11): 1089–1118. doi:10.1007/s12630-013-0019-3
- 13. Heidegger T. Management of the difficult airway. N Engl J Med. 2021; 384: 1836–1847. doi:10.1056/NEJMra1916804
- 14. Ovassapian A. Fiberoptic endoscopy and the difficult airway. Anesth Clin North Am. 2002; 20(4): 755–776. doi:10.1016/S0889-8537(02)00018-1.
- 15. Xue F.S., Li C.W., Liu K.P., Zhang G.H., Yang Q.Y., Xu Y.C. Circulatory responses to fiberoptic intubation in anesthetized patients: comparison of oral and nasal routes. J Clin Anesth. 2007; 19(3): 168–172. doi:10.1016/j.jclinane.2006.09.010.
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
Conflicts of Interest
No conflicts of interest in this work.
About this article
Cite this article
Sanjay Kumar, Rekha Kumari, Rajesh Kumar, et al. Awake Fibreoptic Intubation for Airway Management in Massive Thyroid Enlargement: A Case Report. Ind J Anesth Analg. 2026; 13(2): 106-110.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license
enables reusers to distribute, remix, adapt, and build upon the material in any
medium or format for noncommercial purposes only, and only so long as
attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| March 03, 2026 | April 07, 2026 | June 30, 2026 |
DOI: https://doi.org/10.21088/ijaa.2349.8471.13226.10
Keywords
Awake fibreoptic intubationDifficult airwayMassive thyroid enlargementTracheal deviationAirway topicalisationThyroid surgerySearch for Similar Articles
Similar Articles
- A Case of Thoracotomy with One Lung Ventilation for Carcinoma Oesophagus
- A Case of Empyema for Thoracotomy and Decortication-Anaesthesia Management
- Full Mouth Rehabilitation in a 3-Year-Old Female Child with Repaired Tetralogy o...
- Do Gel Manicures Affect SpO2 Readings ? A Clinical Investigation
- Nebulized Dexmedetomidine Versus Lignocaine for Attenuation of Hemodynamic Respo...
Article Level Metrics
Last UpdatedMonday 27 July 2026, 17:05:43 (IST)
6248
Accesses
20
720
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | March 03, 2026 |
| Accepted | April 07, 2026 |
| Published | June 30, 2026 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license
enables reusers to distribute, remix, adapt, and build upon the material in any
medium or format for noncommercial purposes only, and only so long as
attribution is given to the creator.