Full Text (PDF)
Journal of Cardiovascular Medicine and Surgery 10(1-2):p 45-50, January – June 2024. | DOI: http://dx.doi.org/10.21088/jcms.2454.7123.10(1-2)24.8
Case Report
Cardioembolic Stroke as an Initial Presentation of Carney's Complex: A Case Report
Aamir Mohammad, Syed Shamayal Rabbani, Hamid Ashraf, Ahmad Alam, Mohd Azam Haseen
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)Rabbani SS, Mohammad A, Ashraf H, et al. Cardioembolic stroke as an initial presentation of Carney's complex: a case report. J Cardiovasc Med Surg. 2024;10(1-2):45-50.
Journal of Cardiovascular Medicine and Surgery 10(1-2):p 45-50, January – June 2024. | DOI: http://dx.doi.org/10.21088/jcms.2454.7123.10(1-2)24.8
How Cite This Article:
Rabbani SS, Mohammad A, Ashraf H, et al. Cardioembolic stroke as an initial presentation of Carney's complex: a case report. J Cardiovasc Med Surg. 2024;10(1-2):45-50.Timeline
Received : April 28, 2024
Accepted : June 16, 2024
Published : June 24, 2024
Abstract
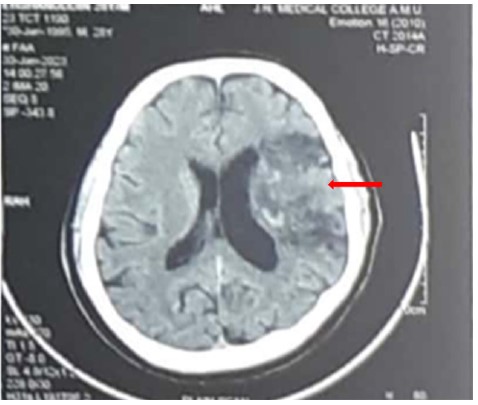
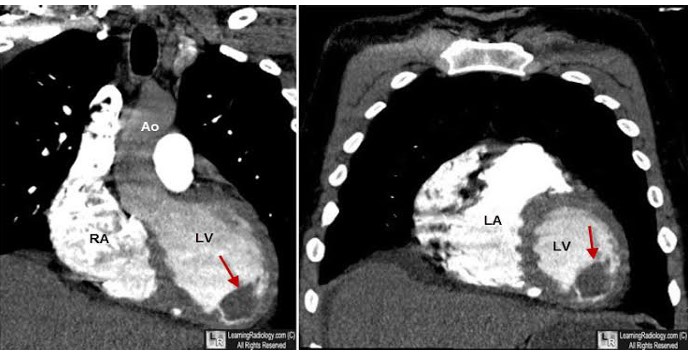
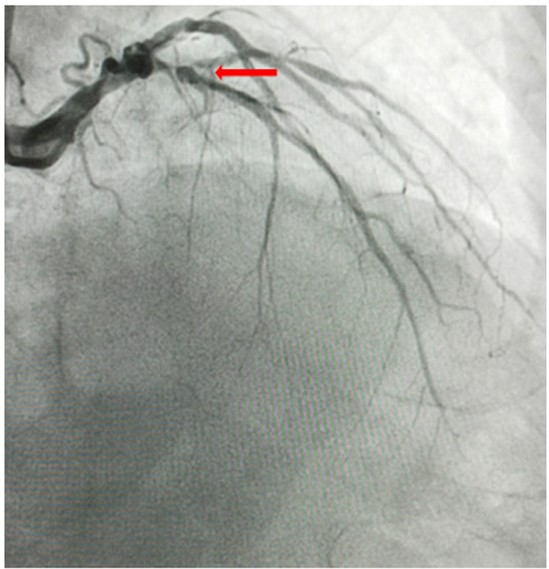
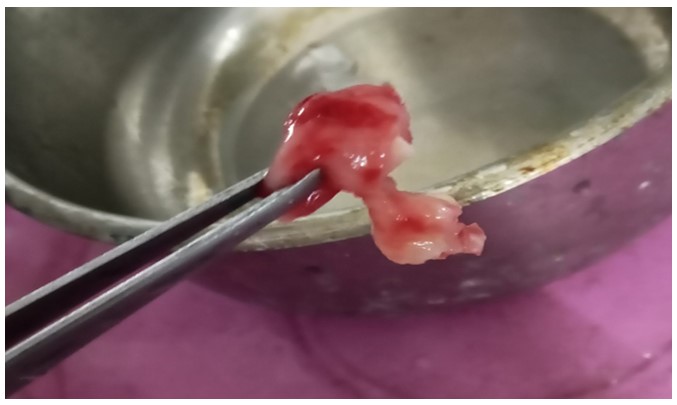
Carney Complex (CNC) is a hereditary lentiginosis syndrome caused by mutations in the PRKAR1A gene, leading to abnormalities in the cyclic AMP-dependent protein kinase (PKA) signalling pathway. This condition predisposes individuals to pigmented lesions, myxomas, and endocrine tumors. We present a case of a 28-year-old male diagnosed with CNC after experiencing a cardioembolic stroke due to a left ventricular myxoma. The diagnosis was suspected following a clinical examination that revealed small, well-demarcated, light brown skin lesions around the eyes and over the back. These characteristic skin findings, combined with the presence of cardiac myxomas, raised the suspicion of CNC. Although CNC typically presents with endocrine abnormalities, this case exemplifies a less common presentation. Our report emphasizes the importance of recognizing the diverse phenotypic spectrum of CNC and the need for awareness of this rare, often under diagnosed syndrome.
References
- 1. Stratakis CA, Kirschner LS, Carney JA. Clinical and molecular features of the Carney complex: diagnostic criteria and recommendations for patient evaluation. J Clin Endocrinol Metab. 2001 Sep;86(9):4041-6. doi: 10.1210/jcem.86.9.7903. PMID: 11549623.
- 2. Stratakis CA. Carney Complex. 2003 Feb 5 [Updated 2023 Sep 21]. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 2024-1993.
- 3. Chatzikonstantinou S, Kazis D, Giannakopoulou P, Poulios P, Pikou O, Geroukis T, Lyssikatos C, Stratakis CA, Bostanjopoulou S. Carney complex syndrome manifesting as cardioembolic stroke: a case report and review of the literature. Int J Neurosci. 2022 Jul;132(7):649-655. doi: 10.1080/00207454.2020.1834393. Epub 2020 Nov 10. PMID: 33027596.
- 4. Nomoto N, Tani T, Konda T, Kim K, Kitai T, Ota M, Kaji S, Imai Y, Okada Y,Furukawa Y. Primary and metastatic cardiac tumors: echocardiographic diagnosis,treatment and prognosis in a 15-years single center study. J CardiothoracSurg. 2017 Nov 28;12(1):103.
- 5. Centofanti P, Di Rosa E, Deorsola L, Dato GM, Patane F, La Torre M, et al.Primary cardiac tumors: early and late results of surgical treatment in 91 patients.Ann Thorac Surg. 1999;68:1236–41.
- 6. Bireta C, Popov AF, Schotola H, Trethowan B, Friedrich M, El-Mehsen M,Schoendube FA, Tirilomis T. Carney-Complex: multiple resections of recurrentcardiac myxoma. J Cardiothorac Surg. 2011 Feb 3;6:12. doi: 10.1186/1749-8090-6-12. PMID: 21291531; PMCID: PMC3038896.
- 7. Kuyama N, Hamatani Y, Fukushima S, Ikeda Y, Nakai E, Okada A, Takahama H, Amaki M, Hasegawa T, Sugano Y, Kanzaki H, Fujita T, Ishibashi-Ueda H, Yasuda S, Anzai T, Kobayashi J. Left ventricular myxoma with Carney complex. ESC Heart Fail. 2018 Aug;5(4):713-715. doi: 10.1002/ ehf2.12282. Epub 2018 Mar 15. PMID: 29542870; PMCID: PMC6073037.
- 8. Briassoulis G, Kuburovic V, Xekouki P, Patronas N, Keil MF, Lyssikatos C, Stajevic M, Kovacevic G, Stratakis CA. Recurrent left atrial myxomas in Carney complex: a genetic cause of multiple strokes that can be prevented. J Stroke Cerebrovasc Dis. 2012 Nov;21(8):914.e1-8. doi: 10.1016/j.jstrokecer ebrovasdis.2012.01.006. Epub 2012 Feb 15. PMID: 22341669; PMCID: PMC3369015.
Data Sharing Statement
There are no additional data available.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval
Acknowledgements
Information Not Provided
Conflicts of Interest
No conflicts of interest in this work.
About this article
Cite this article
Rabbani SS, Mohammad A, Ashraf H, et al. Cardioembolic stroke as an initial presentation of Carney's complex: a case report. J Cardiovasc Med Surg. 2024;10(1-2):45-50.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)Rabbani SS, Mohammad A, Ashraf H, et al. Cardioembolic stroke as an initial presentation of Carney's complex: a case report. J Cardiovasc Med Surg. 2024;10(1-2):45-50.
| Received | Accepted | Published |
|---|---|---|
| April 28, 2024 | June 16, 2024 | June 24, 2024 |
DOI: http://dx.doi.org/10.21088/jcms.2454.7123.10(1-2)24.8
Keywords
Carney's ComplexCNC typicallyCardioembolic strokeVentricular myxomaCneoplasia syndromeSearch for Similar Articles
Similar Articles
- Giant Intra-cardiac Lipoma in the Right Atrium
- Case Report: Neurophysiological Facilitation of Respiration in an Infant with...
- Left Coronary Artery Fistula Masquerading as Coronary Insufficiency: A Rare Sur...
- Hemodynamic Monitoring by Point-of-Care Ultrasound: A Multiorgan, Physiology-Dri...
- Aortotomy Closure after Cardiac Valve Replacements: Nightmare for Surgeons
Article Level Metrics
Last UpdatedFriday 31 July 2026, 00:54:49 (IST)
1015
Accesses
7
136
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | April 28, 2024 |
| Accepted | June 16, 2024 |
| Published | June 24, 2024 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
Rabbani SS, Mohammad A, Ashraf H, et al. Cardioembolic stroke as an initial presentation of Carney's complex: a case report. J Cardiovasc Med Surg. 2024;10(1-2):45-50.