Full Text (PDF)
Indian Journal of Anesthesia and Analgesia 12(1):p 65-69, Jan- March 2025. | DOI: https://doi.org/10.21088/ijaa.2349.8471.12125.13
Case Report
Anaesthetic Management of Tracheo-oesophageal fistula/oesophageal atresia in Neonate
Matcha Reddysri, Ravi Madhusudhana, Revathi A., Namratha K.
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Anesthesia and Analgesia 12(1):p 65-69, Jan- March 2025. | DOI: https://doi.org/10.21088/ijaa.2349.8471.12125.13
How Cite This Article:
Reddysri M, Madhusudhana R, Revathi A., et. al, Anaesthetic Management of Tracheo-oesophageal fistula/ oesophageal atresia in Neonate. Ind J Anesth Analg. 2025; 12(1): 65-69.Timeline
Received : January 10, 2025
Accepted : February 13, 2025
Published : March 15, 2025
Abstract
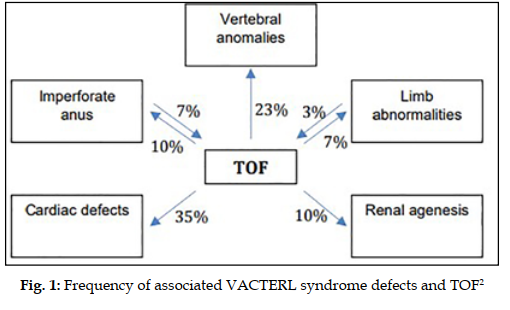
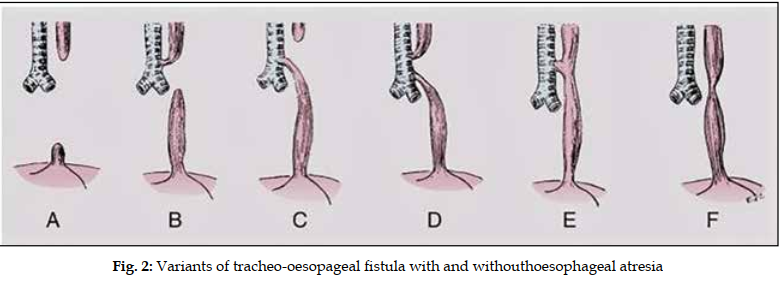
Introduction: Tracheo-oesophageal fistula with or without oesophageal atresia is a congenital anomaly with an incidence of 1 in 3000-4000 births worldwide. Although congenital cardiac disease is the most frequent congenital anomaly, up to 50% of infants have TOF in addition to other congenital abnormalities. Case Report: At 3 day old the baby was planned for one lung ventilation with right thoracotomy + trachea-oesophageal repair in view of trachea-oesophageal fistula with oesophageal atresia. On examination, the general condition of the child was poor. He was tachypneic with a respiratory rate of 62/min along with chest retraction and nasal flaring. In the operating room, standard monitors were attached. Two intravenous line was secured with 24-gauge cannula on both dorsum of hands. Intravenous anesthesia drugs were loaded using insulin syringe according to baby’s weight. Induced with ketamine 4 mg and fentany l4 μg. After confirmation of bag and mask ventilation, succinylcholine 4 mg was given to facilitate end otracheal intubation. Trachea was intubated successfully with uncuffed endotracheal tube of internal diameter 3.0 mm confirmed by auscultation of chest and capnography. The child was ventilated with low tidal volume and high rate. Anesthesia was maintained with oxygen, isoflurane and atracurium. The child was positioned in the right lateral position and thoracotomy was done. At the end of surgery, trial of extubation was done and due to insufficient respiratory effort baby was shifted with ET tube in-situ to NICU. Conclusion: The anesthetic approach for neonates with TEF with or without EA should primarily concentrate on airway management and ventilation techniques. Maintaining airway patency, ensuring proper ventilation, and adequate oxygenation rely on effective communication between the pediatric surgeon and the anesthetist during the procedure Neonates are typically recommended to remain intubated endotracheally for a specific duration following surgery, necessitating the arrangement of an NICU bed in advance for these infants before definitive repair.
References
- 1. Hunt R.W., Perkins E.J., King S. Peri-operative management of neonates with oesophageal atresia and tracheo-oesophageal fistula. Paediatr Respir Rev 2016; 19: 3-9.
- 2. Goyal, A; Jones, M.O; Couriel, J.M.; Losty, P.D. Oesophagealatresia and trachea-oesophageal fistula. Archives of Diseasein Childhood-Fet al. and Neonatal Edition. 2006; 91(5) F381-F384.
- 3. Mwesige S., Ngotta V., Ngowi N., Salim M. A successful repair of esophageal atresia (EA) with distal tracheoesophageal fistula (TEF) to a 6-day-old child in a low-resource setting. Case report. Int J Surg Case Rep. 2023 Dec; 113: 109065. doi: 10.1016/j.ijscr.2023.109065. Epub 2023 Nov 17. PMID: 37979557; PMCID: PMC10694280.
- 4. Cuestas G., Rodríguez V., Millán C., Bellia Munzón P., Bellia Munzón G. H-type tracheoesophageal fistula in the neonatal period: Difficulties in diagnosis and different treatment approaches. A case series. Arch Argent Pediatr. 2020 Feb; 118(1): 56-60. English, Spanish. doi: 10.5546/aap.2020.eng.56. PMID: 31984700.
- 5. Beasley S.W., Shann F.A., Myers N.A., Auldist A.W. Developments in the management of oesophageal atresia and tracheo-oesophageal fistulas. Med J Aust. 1989 May 1; 150(9): 501- 3. doi: 10.5694/j.1326-5377.1989.tb136595.x. PMID: 2725405.
Data Sharing Statement
There are no additional data available.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
Information not provided.
Conflicts of Interest
The authors report no conflicts of interest in this work.
About this article
Cite this article
Reddysri M, Madhusudhana R, Revathi A., et. al, Anaesthetic Management of Tracheo-oesophageal fistula/ oesophageal atresia in Neonate. Ind J Anesth Analg. 2025; 12(1): 65-69.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| January 10, 2025 | February 13, 2025 | March 15, 2025 |
DOI: https://doi.org/10.21088/ijaa.2349.8471.12125.13
Keywords
Airway managementEsophagealatresia (EA)Tracheoesophageal fistula (TEF)Neonate anesthesiaSearch for Similar Articles
Similar Articles
- Awake Fibreoptic Intubation for Airway Management in Massive Thyroid Enlargement...
- A Case of Thoracotomy with One Lung Ventilation for Carcinoma Oesophagus
- A Case of Empyema for Thoracotomy and Decortication-Anaesthesia Management
- Full Mouth Rehabilitation in a 3-Year-Old Female Child with Repaired Tetralogy o...
- Do Gel Manicures Affect SpO2 Readings ? A Clinical Investigation
Article Level Metrics
Last UpdatedTuesday 14 July 2026, 17:03:34 (IST)
5702
Accesses
11
679
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | January 10, 2025 |
| Accepted | February 13, 2025 |
| Published | March 15, 2025 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.