Full Text (PDF)
Indian Journal of Anesthesia and Analgesia 9(3):p 131-134, May-June 2022. | DOI: https://doi.org/10.21088/ijaa.2349.8471.9322.12
Case Report
Anaesthetic Management of Patient with Hypertrophy Obstructive Cardiomyopathy Posted for Elective Caesarean
Ravi Madhusudhana null, Pooja Arunkumar Giriyapur 1 null, Ravi Madhusudhana 2 null, Sumanth Tarigonda 3 null, Sravanthi Nagasai Ganagavarapu 4 null
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to
distribute, remix, adapt, and build upon the material in any medium or format
for noncommercial purposes only, and only so long as attribution is given to
the creator.
Indian Journal of Anesthesia and Analgesia 9(3):p 131-134, May-June 2022. | DOI: https://doi.org/10.21088/ijaa.2349.8471.9322.12
How Cite This Article:
Pooja Arunkumar Giriyapur, Ravi Madhusudhana, Sumanth Tarigonda, et al./Anaesthetic Management of Patient with Hypertrophy Obstructive Cardiomyopathy Posted for Elective Caesarean/Indian J Anesth Analg. 2022;9(3):131-
134.
Timeline
Received : April 10, 2022
Accepted : May 03, 2022
Published : June 20, 2022
Abstract
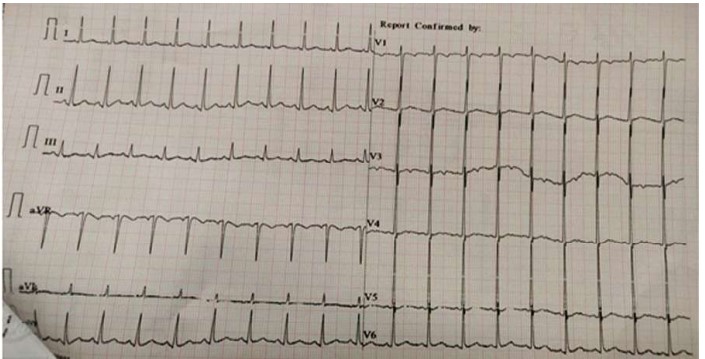
Introduction: Dynamic valvular insufficiency and LVOT blockage are also possible outcomes of hypertrophic obstructive cardiomyopathy (HOCM). Furthermore, attempting to replace an inadequate mitral valve surgically can result in iatrogenic LVOT blockage. In the general population, it affects one out of every 500 adults, with a male to female ratio of 2:1. Among the general population, the prevalence is around 0.2 percent, and the incidence in pregnant women is around 0.1–0.5 percent. Case Report: 21 year old female patient presented with 9 months of amenorrhea posted for elective lower segment caesarean section. Her previous documents revealed that she was a diagnosed case of hypertrophic obstructive cardiomyopathy during her last pregnancy 1 year ago. History of previous surgery that is induced abortion at two and half months of gestation age a year back operated under spinal anaesthesia. ECG showed ST elevation present in V2 , V3, V4 , V5 leads and features of left ventricular hypertrophy (LVH) , Her echocardiography report revealed features of hypertrophic obstructive cardiomyopathy with severe LVOT obstruction. Left ventricular ejection fraction (LVEF) was 20-25%. Conclusion: HOCM is normally well tolerated during pregnancy, although those who have had previous symptoms or arrhythmias may experience an exacerbation of symptoms. The majority of these people, on the other hand, can be effectively controlled medically. This case report showed that patients with HOCM can be safely managed under general anaesthesia with muscle relaxants and inhalational volatile anaesthetics, as well as an erector spinae block for analgesia
References
- 1. Bhalerao PM, Adsule PB, Marathe RM: Anaesthetic management of a patient with hypertrophic obstructive cardiomyopathy posted for emergency lower segment caesarean section. J Obstet Anaesth Crit Care.
- 2. Bhure AR, Marodkar KS: Successful anaesthetic management of a case of hypertrophic obstructive
- 3. Pieper PG, Walker F: Pregnancy in women with hypertrophic cardiomyopathy. Neth Heart J. 2013, 21:14-18.
- 4. Sahoo RK, Dash SK, Raut PS, Badole UR, Upasani CB: Perioperative anesthetic management of patients with hypertrophic cardiomyopathy for noncardiac surgery: A case series. Ann Card Anaesth. 2010, 13:253-6.
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
Provide information related to the Ethics Committee approval with approval number OR write, This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
Conflicts of Interest
The authors report no conflicts of interest in this work.
About this article
Cite this article
Pooja Arunkumar Giriyapur, Ravi Madhusudhana, Sumanth Tarigonda, et al./Anaesthetic Management of Patient with Hypertrophy Obstructive Cardiomyopathy Posted for Elective Caesarean/Indian J Anesth Analg. 2022;9(3):131-
134.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to
distribute, remix, adapt, and build upon the material in any medium or format
for noncommercial purposes only, and only so long as attribution is given to
the creator.
| Received | Accepted | Published |
|---|---|---|
| April 10, 2022 | May 03, 2022 | June 20, 2022 |
DOI: https://doi.org/10.21088/ijaa.2349.8471.9322.12
Keywords
ErectorspinaeblockEsmololCMeartdiseaseInhalationalanaestheticsPregnancy.Pregnancy.Search for Similar Articles
Similar Articles
- Awake Fibreoptic Intubation for Airway Management in Massive Thyroid Enlargement...
- A Case of Thoracotomy with One Lung Ventilation for Carcinoma Oesophagus
- A Case of Empyema for Thoracotomy and Decortication-Anaesthesia Management
- Full Mouth Rehabilitation in a 3-Year-Old Female Child with Repaired Tetralogy o...
- Do Gel Manicures Affect SpO2 Readings ? A Clinical Investigation
Article Level Metrics
Last UpdatedTuesday 14 July 2026, 10:56:13 (IST)
5693
Accesses
11
679
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | April 10, 2022 |
| Accepted | May 03, 2022 |
| Published | June 20, 2022 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to
distribute, remix, adapt, and build upon the material in any medium or format
for noncommercial purposes only, and only so long as attribution is given to
the creator.