Full Text (PDF)
Indian Journal of Anesthesia and Analgesia 12(3):p 234-238, July-Sept. 2025. | DOI: https://doi.org/10.21088/ijaa.2349.8471.12325.10
Case Report
Anaesthetic Management of Morgagni’s Hernia Repair with Coronary Artery Bypass Grafting Surgery
Anirudh Thimmangouda Patil, Abhijeet B. Shitole, Sharanagouda Patil, Anand Vagarali, Jabbar Momin, Sweta Sooragonda, Rajesh Munigial
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Anesthesia and Analgesia 12(3):p 234-238, July-Sept. 2025. | DOI: https://doi.org/10.21088/ijaa.2349.8471.12325.10
How Cite This Article:
Patil AT, Shitole AB, et al. Anaesthetic management of Morgagni’s hernia repair with coronary artery bypass grafting surgery. Ind J Anesth Analg. 2025;12(3):234-238.Timeline
Received : April 05, 2025
Accepted : June 05, 2025
Published : September 11, 2025
Abstract
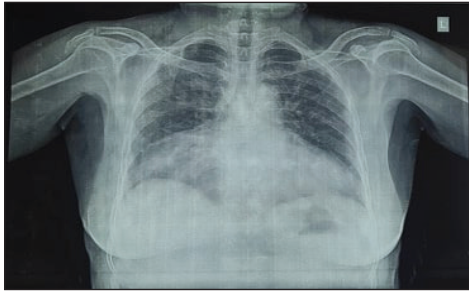
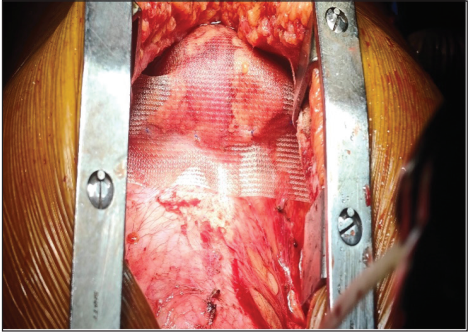
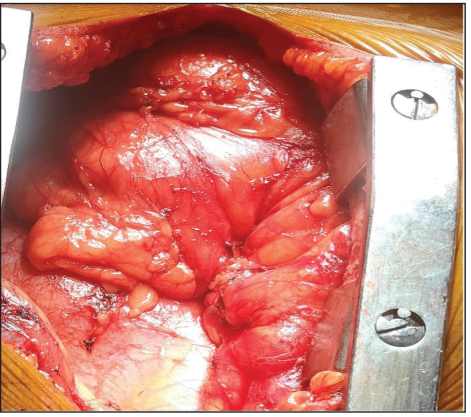
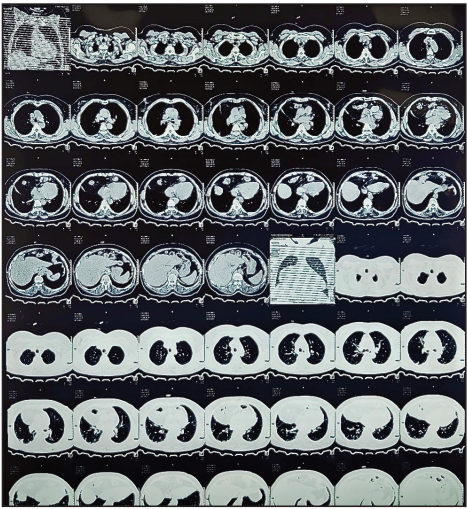
A 60-year-old female patient presented with breathlessness (NYHA grade II), retrosternal chest pain, and postprandial fullness, alongside heartburn symptoms. Clinical evaluation revealed prominent Q waves and ST-segment depression on ECG, while chest X-ray showed a raised right-sided hemidiaphragm with bowel loop shadows, suggesting a diaphragmatic hernia or eventration. Pulmonary function tests were unremarkable. An echocardiogram indicated a dysfunctional left ventricle with an ejection fraction of 45%, apical septal akinesia, inferior wall hypokinesia, and mild mitral regurgitation. CT imaging of the chest and abdomen confirmed a diaphragmatic defect with herniation of omental fat and a large portion of the transverse colon, causing atelectasis of the medial right middle lobe. Coronary angiography revealed lesions in the left anterior descending artery, left circumflex artery, and right coronary artery. The patient was diagnosed with both coronary artery disease and diaphragmatic hernia and was recommended for coronary artery bypass grafting (CABG) along with diaphragmatic hernia repair. Intraoperatively, the patient was managed with standard ASA monitors, rapid sequence induction, and a left-sided double-lumen tube for single-lung ventilation. The hernia was repaired with polypropylene mesh, and CABG was performed offpump after achieving adequate anticoagulation. Postoperatively, the patient showed improvement with a significant reduction in airway pressure and was extubated 8 hours post-surgery. Bowel sounds were audible by postoperative day 1, and the patient was discharged on the 7th postoperative day without complications. This case highlights the complexity of managing concomitant coronary artery disease and diaphragmatic hernia, emphasizing a multidisciplinary approach to treatment and anesthesia.
References
- 1. Pranata H., Kurniyanta P. Anesthesia management of congenital diaphragmatic hernia in neonates. Bali Journal of Anesthesiology. 2021 Jan 1; 5(1): 53-6.
- 2. Kulkarni K., Patil S., Mubarizuddin A., Malager A. Management of congenital diaphragmatic hernia with epidural and general anaesthesia. J Anesth Clin Care. 2018; 5: 30.
- 3. McGovern R., McGovern V., Healy M. Congenital diaphragmatic hernias-part 2. WFSA. 2024.
- 4. Paliwal S., Lewis B., Kaufman IV H. Congenital diaphragmatic hernia in an 81-year-old female presenting as painless jaundice: a case report. International Journal of Surgery Case Reports. 2022 Jun 1; 95: 107238.
- 5. Sellke F., Del Nido P.J., Swanson S.J. Sabiston and Spencer’s Surgery of the Chest E-Book. Elsevier Health Sciences; 2009 Dec 16.
- 6. Quinney M., Wellesley H. Anaesthetic management of patients with a congenital diaphragmatic hernia. BJA education. 2018 Apr 1; 18(4): 95-101.
- 7. Mohan G., Kalyanaraman S., Ramakrishnan S., Theodore S. Concomitant diaphragmatic hernia repair with coronary artery bypass grafting surgery. Annals of Cardiac Anaesthesia Internet. 2018 Jan 1; 21(3): 304. Available from: https://doi.org/10.4103/aca.aca_42_17.
- 8. Mar Fan M.J., Coulson M.L., Siu S.K. Adult Incarcerated Right-Sided Bochdalek Hernia. Australian and New Zealand journal of surgery. 1999 Mar; 69(3): 239-41.
- 9. Stankiewicz B., Mierzewska-Schmidt M., Pałko K.J., Baranowski A., Darowski M., Kozarski M. A new method of ventilation inhomogeneity assessment based on A simulation study using clinical data on congenital diaphragmatic hernia cases. Scientific Reports. 2022 Dec 31; 12(1): 22635.
- 10. Gahlot D., Saxena K.N., Wadhwa B. Anaesthetic Management of Non Traumatic Diaphragmatic Hernia as a Co-existing Disease: Combined Spinal Epidural to Rescue. Journal of Clinical & Diagnostic Research. 2021 Jun 1; 15(6).
- 11. Williams D.J., Sandby-Thomas M.G. Anaesthetic management of acute gastric volvulus in an adult. British journal of anaesthesia. 2003 Jan 1; 90(1): 96-8.
- 12. Reddy A.A., Ayyan S.M., Anandhi D., Ganessane E., Amrithanand V.T. Bed-uphead-elevated Position versus Supine Sniffing Position in Patients Undergoing Rapid Sequence Intubation Using Direct Laryngoscopy in the Emergency Department–A Randomized Controlled Trial. Journal of Emergencies, Trauma, and Shock. 2024 Apr 1; 17(2): 58-65.
Data Sharing Statement
There are no additional data available.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
Information not provide.
Conflicts of Interest
The authors report no conflicts of interest in this work.
About this article
Cite this article
Patil AT, Shitole AB, et al. Anaesthetic management of Morgagni’s hernia repair with coronary artery bypass grafting surgery. Ind J Anesth Analg. 2025;12(3):234-238.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| April 05, 2025 | June 05, 2025 | September 11, 2025 |
DOI: https://doi.org/10.21088/ijaa.2349.8471.12325.10
Keywords
AnaesthesiologyCardiac AnaesthesiologyCongenital diaphragmatic herniaMorgagnis herniaAnaesthesiaSearch for Similar Articles
Similar Articles
- Awake Fibreoptic Intubation for Airway Management in Massive Thyroid Enlargement...
- A Case of Thoracotomy with One Lung Ventilation for Carcinoma Oesophagus
- A Case of Empyema for Thoracotomy and Decortication-Anaesthesia Management
- Full Mouth Rehabilitation in a 3-Year-Old Female Child with Repaired Tetralogy o...
- Do Gel Manicures Affect SpO2 Readings ? A Clinical Investigation
Article Level Metrics
Last UpdatedTuesday 14 July 2026, 10:02:56 (IST)
5690
Accesses
10
679
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | April 05, 2025 |
| Accepted | June 05, 2025 |
| Published | September 11, 2025 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.