Full Text (PDF)
Journal of Cardiovascular Medicine and Surgery 9(3-4):p 43-47, July-December 2023. | DOI: http://dx.doi.org/10.21088/jcms.2454.7123.93-423.1
Original Article
Role of Half Dose Tenecteplase in Submassive Pulmonary Embolism: Analysis of A Case Report
Edmond Nyaribo, Timothy Wachira, Charles Masese, Anthony Gikonyo, Loise Ndunge, Premanand Ponoth, Duncan Luvayo
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator
Journal of Cardiovascular Medicine and Surgery 9(3-4):p 43-47, July-December 2023. | DOI: http://dx.doi.org/10.21088/jcms.2454.7123.93-423.1
How Cite This Article:
Nyaribo E, Ndunge L, Gikonyo A, Masese C, Wachira T, Luvayo D, et al. Role of half dose tenecteplase in submassive pulmonary embolism: analysis of a case report. J Cardiovasc Med Surg. 2023;9(3-4):43–7.Timeline
Received : August 30, 2023
Accepted : September 30, 2023
Published : December 30, 2023
Abstract
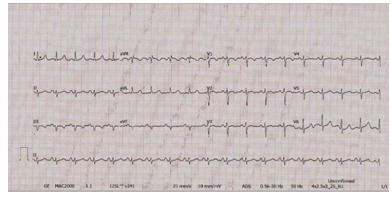
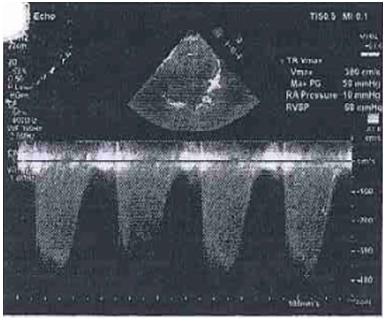
Background: Initial assessment of acute Pulmonary Embolism (PE) is essential in risk stratification into low-risk and high-risk (massive) Pulmonary embolism as per the hemodynamic stability. Patients with submassive PE who are likely to progress for hemodynamic instability should receive anticoagulation and should be monitored. Method: This is a descriptive case report of a 45-year-old female who presented with history of nonproductive cough for 2 weeks, associated with retrosternal chest pain and shortness of breath. On physical exam her vitals were: temp 38.1 degrees Celsius, BP 160/106mmhg, SPO 2 84% on room air, pulse 113b/min, R/R 26 cycles/min. She had distended neck veins with vigorous pulsation seen JVP 10mmhg. On auscultation there was reduced air entry and a systolic murmur in left sternal border, D dimer >6000ng/dl (0-500ng/dl), cardiac troponin 0.6ng/ml. Computerized tomography pulmonary angiogram (CTPA) revealed bilateral pulmonary emboli in the right and left pulmonary arteries and an echo suggestive of severe pulmonary arterial hypertension with a peak value of > 70mmhg with preserved left ventricular ejection fraction (LVEF) 57%. Results: Successful thrombolysis was achieved with half dose Tenecteplase. There was no bleeding during and after Tenecteplase administration. The patient was discharged on the 4th day in stable condition. Discussion: Half-dose thrombolysis with Tenecteplase has shown to improve pulmonary perfusion resulting in improved clinical symptoms and a short hospital stay with minimal chance for bleeding issues. Patients with sub massive PE at highest risk for progression to hemodynamic instability should receive anticoagulation and be monitored for clinical deterioration. Conclusion: Low-dose Tenecteplase is therefore a safe and efficacious treatment option for sub massive PE as denoted. However, larger randomized controlled trials are needed to establish low-dose Tenecteplase as an accepted treatment modality
References
- 1. Turetz, M., Sideris, A.T., et al. (2018) Epidemiology, Pathophysiology, and Natural History of Pulmonary Embolism. Semin Intervent Radio
- 2. Danwang, C., Temgoua, M.N., et al (2017) Epidemiology of venous thromboembolism in Africa: a systematic review. Journal of Thrombosis and Haemostasishttps://pubmed.ncbi.nlm.nih.gov/2879 6427/
- 3. Ogeng'o, J.A., Obimbo, M.M., et al. (2011) Pulmonary thromboembolism in an East African tertiary referral hospital. Journal of Thrombosis and Thrombolysis https://pubmed.ncbi.nlm.nih.gov/21674133/
- 4. Igneri, L.A., Hammer, J.M. (2018) Systemic Thrombolytic Therapy for Massive and Submassive Pulmonary Embolism. Journal of Pharmacy Practicehttps://pubmed.ncbi.nlm.nih.gov/29673293/
- 5. Zhang, Z., Xi, L., et al (2022) Tenecteplase in Pulmonary Embolism Patients: A Meta-Analysis and Systematic Review. National Library of Medicine https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC9008780/
- 6. Yilmaz, E.S., Uzun, O. (2021) Low-dose thrombolysis for submassive pulmonary embolism. National Library of Medicine. https://pubmed.ncbi.nlm.nih. gov/34099544/
- 7. Weng, C., Wang, X., et al (2021) Low-dose urokinase thrombolytic therapy for patients with acute intermediate-high-risk pulmonary embolism: A retrospective cohort study.. National Library of Medicine. https://www.ncbi.nlm.nih.gov/pmc/ articles/PMC7997002/
Data Sharing Statement
There are no additional data available
Funding
This research received no funding
Author Contributions
All authors contributed significantly to the work and approve its publication
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval
Acknowledgements
Information Not Provided
Conflicts of Interest
No conflicts of interest in this work.
About this article
Cite this article
Nyaribo E, Ndunge L, Gikonyo A, Masese C, Wachira T, Luvayo D, et al. Role of half dose tenecteplase in submassive pulmonary embolism: analysis of a case report. J Cardiovasc Med Surg. 2023;9(3-4):43–7.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator
| Received | Accepted | Published |
|---|---|---|
| August 30, 2023 | September 30, 2023 | December 30, 2023 |
DOI: http://dx.doi.org/10.21088/jcms.2454.7123.93-423.1
Keywords
ThrombolysisPulmonary embolismPESearch for Similar Articles
Similar Articles
- Giant Intra-cardiac Lipoma in the Right Atrium
- Case Report: Neurophysiological Facilitation of Respiration in an Infant with...
- Left Coronary Artery Fistula Masquerading as Coronary Insufficiency: A Rare Sur...
- Hemodynamic Monitoring by Point-of-Care Ultrasound: A Multiorgan, Physiology-Dri...
- Aortotomy Closure after Cardiac Valve Replacements: Nightmare for Surgeons
Article Level Metrics
Last UpdatedFriday 31 July 2026, 14:14:33 (IST)
1019
Accesses
7
136
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | August 30, 2023 |
| Accepted | September 30, 2023 |
| Published | December 30, 2023 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator