Full Text (PDF)
Indian Journal of Medical and Health Sciences 11(2):p 47-58, Oct - Dec. 2024. | DOI: https://doi.org/10.21088/ijmhs.2347.9981.11224.1
Original Article
Risk Factors, Clinical Profile, Outcome in Hypertensive Crisis
Venkatesh V. Madholli, Shashibhushan J., Raghavendra F.N., Lngaraja null
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Medical and Health Sciences 11(2):p 47-58, Oct - Dec. 2024. | DOI: https://doi.org/10.21088/ijmhs.2347.9981.11224.1
How Cite This Article:
Shashibhushan J., Venkatesh V. Madholli et al., Risk Factors, Clinical Profile, Outcome in Hypertensive Crisis. Jr. Med. & Health Sci. 2024;11(2):47–58Timeline
Received : October 21, 2024
Accepted : November 22, 2024
Published : December 30, 2024
Abstract
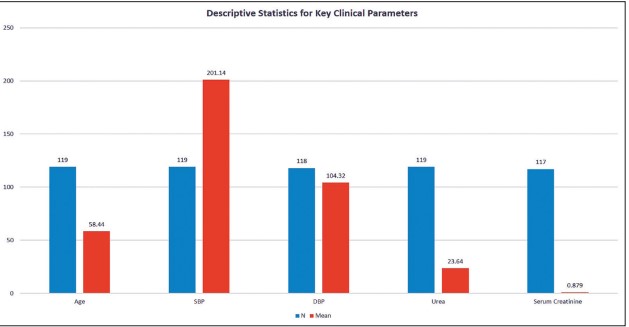
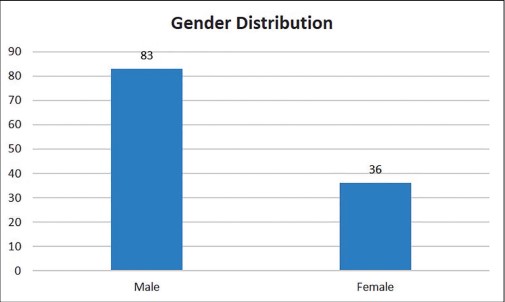
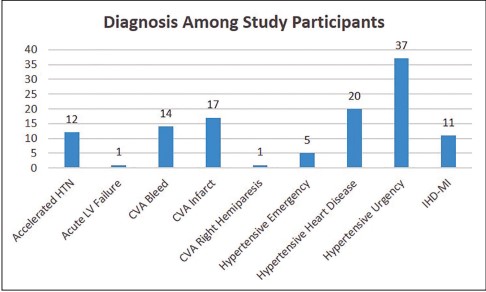
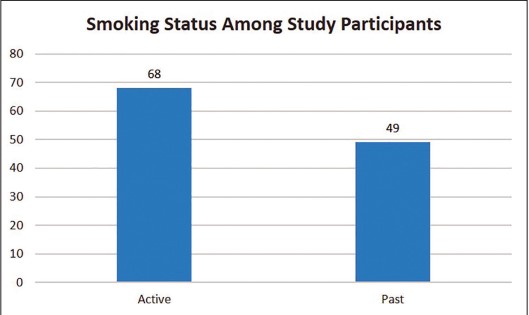
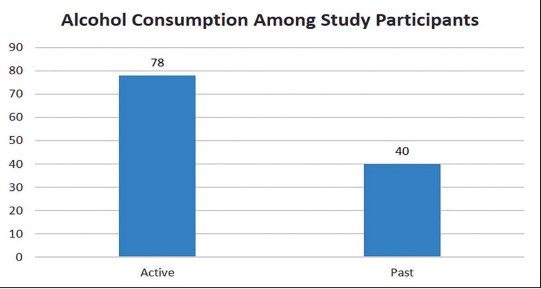
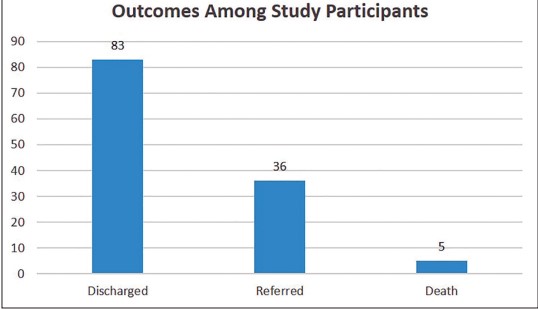
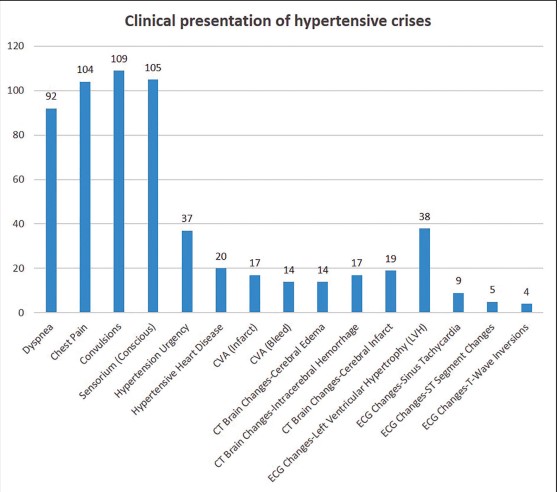
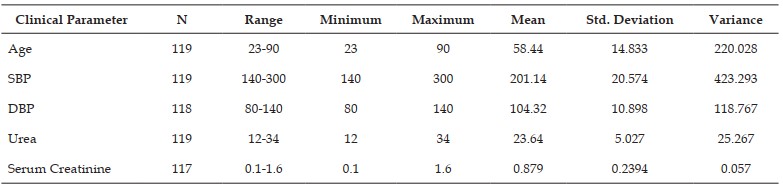
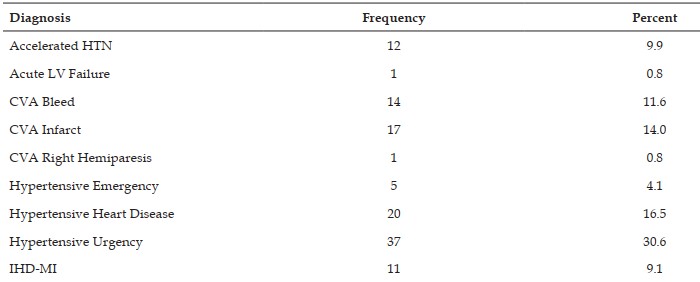
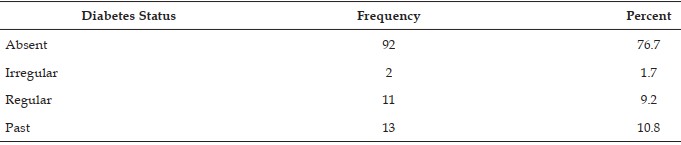
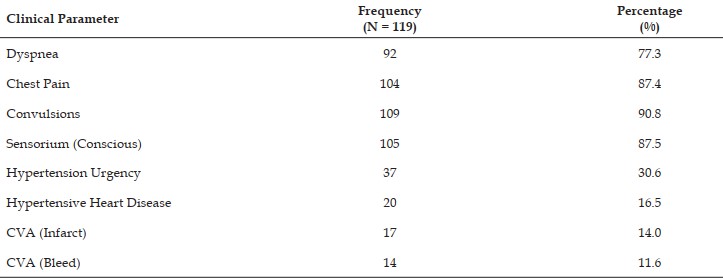
Background: Hypertensive crises, including hypertensive urgency and emergency, are lifethreatening conditions characterized by severely elevated blood pressure. This study aimed to investigate the risk factors, clinical profile, and outcomes among patients presenting with hypertensive crises at Bellary Medical College And Research center Bellary, India. Methods: A prospective descriptive study was conducted, involving 119 patients aged 18 years and above with systolic blood pressure ≥180 mmHg or diastolic blood pressure ≥110 mmHg, along with evidence of target organ damage. Patients with secondary causes of hypertension were excluded. Data collection included demographic characteristics, clinical presentation, blood pressure measurements, and diagnostic tests such as CT brain scans and ECGs. Descriptive statistics were used to summarize key variables, and statistical tests assessed associations between clinical findings and outcomes. Results: The mean age of the patients was 58.44 years, with 69.2% being male. The mean systolic blood pressure was 201.14 mmHg, and the mean diastolic blood pressure was 104.32 mmHg. The most common diagnosis was hypertensive urgency (30.6%), followed by hypertensive heart disease (16.5%), and cerebrovascular accidents (CVA-infarct: 14.0%, CVA-bleed: 11.6%). Active smoking was reported in 56.7% of patients, and 65.0% were active alcohol consumers. A total of 69.7% of patients were discharged, 30.3% were referred for further care, and the mortality rate was 4.2%. Conclusions: Hypertensive crises are associated with significant morbidity, particularly in male patients and those with lifestyle risk factors such as smoking and alcohol consumption. Stroke, heart disease, and renal involvement were common complications. Effective management requires timely blood pressure control and addressing modifiable risk factors to prevent severe outcomes.
References
- 1. Zampaglione B., Pascale C., Marchisio M, Cavallo-Perin P. Hypertensive urgencies and emergencies. Prevalence and clinical presentation. Hypertension. 1996; 27(1):144- 7. doi: 10.1161/01.hyp.27.1.144.
- 2. Pinna G., Pascale C., Fornengo P., Arras S, Piras C., Panzarasa P., et al. Hospital admissions for hypertensive crisis in the emergency departments: a large multicenter Italian study. PLoS One. 2014; 9(4):e93542. doi: 10.1371/journal.pone.0093542.
- 3. Nkoke C., Noubiap J.J., Dzudie A, Jingi AM, Njume E., Nkouonlack C., et al. Epidemiology of hypertensive crisis in the Buea Regional Hospital, Cameroon. J. Clin Hypertens (Greenwich). 2020;22(12):2105-10. doi: 10.1111/jch.14061.
- 4. Gebresillassie B.M., Debay Y.B. Characteristics, treatment, and outcome of patients with hypertensive crisis admitted to University of Gondar Specialized Hospital, northwest Ethiopia: A cross-sectional study. J. Clin Hypertens (Greenwich). 2020;22(12):2343-53. doi: 10.1111/jch.14060.
- 5. Salkic S., Batic-Mujanovic O., Ljuca F., Brkic S. Clinical presentation of hypertensive crises in emergency medical services. Mater Sociomed. 2014; 26(1):12- 6. doi:10.5455/msm.2014.26.12-16.
- 6. Kotruchin P., Pratoomrat W., Mitsungnern T., Khamsai S., Imoun S. Clinical treatment outcomes of hypertensive emergency patients: Results from the hypertension registry program in Northeastern Thailand. J. Clin Hypertens (Greenwich). 2021;23(3):621-7. doi: 10.1111/jch.14119.
- 7. Abou Farha K., van Vliet A., van Marle S., Vrijlandt P., Westenbrink D. Hypertensive crisis-induced electrocardiographic changes: a case series. J. Med Case Rep. 2009; 3:7283. doi: 10.4076/1752-1947-3-7283.
- 8. Singh N., Tarun, Pal R., Chamoli A. Clinical profile of patients with hypertensive crisis presenting to an emergency department of a tertiary care hospital in Haryana, India - A retrospective crosssectional study. Asian J Med Sci. 2022;13(1):59-63. doi: 10.3126/ajms.v13i1.39591.
- 9. Goswami B., Nanda V. Clinical profile of patients with hypertensive crisis presenting to an emergency department of a tertiary care hospital in Western India. Apollo Med. 2023; 21(2):10.4103/am.am_121_23. doi: 10.4103/am.am_121_23.
- 10. Talle M.A., Ngarande E., Doubell A.F., Herbst P.G. Cardiac complications of hypertensive emergency: Classification, diagnosis and management challenges. J. Cardiovasc Dev Dis. 2022;9(8):276. doi: 10.3390/jcdd9080276.
- 11. Kotruchin P., Pratoomrat W., Mitsungnern T., Khamsai S., Imoun S. Clinical treatment outcomes of hypertensive emergency patients: Results from the hypertension registry program in Northeastern Thailand. J Clin Hypertens. 2021; 23:621–7. doi: 10.1111/jch.14119.
- 12. Baumann B.M., Gallagher J.M., Honigman B.K., Sinha M. Dyspnea in hypertensive emergencies: a predictor of poor outcomes. J Emerg Med. 2018; 54(1):37-42.
- 13. Currie J.R., Reiter R.E., Wright D.F., Gunby C.P. Convulsions in hypertensive encephalopathy. Arch Intern Med. 1988; 148(7):1498-500.
- 14. De Luca G., Suryapranata H., Ottervanger J.P., Antman E.M. Chest pain and hypertensive crises: diagnostic and therapeutic considerations. Am Heart J. 2017; 196:10-20.
- 15. Devereux R.B., Pickering T.G., Harshfield G.A., et al. Left ventricular hypertrophy in patients with hypertension: importance of blood pressure response to regularly occurring physical activity. J. Am Coll Cardiol. 1987;9(3):639-48.
- 16. Doll R., Peto R., Boreham J., Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ. 2004;328(7455):1519.
- 17. Li J., Zhu X., Xu S., et al. Giddiness in hypertensive crises: cerebral hypoperfusion and transient ischemic attacks. Neurology. 2020; 94(10).
- 18. Lu T.H., Lee C.H., Chou Y.J. Gender differences in the prevalence and control of hypertension among older adults in Taiwan. J. Clin Hypertens (Greenwich). 2019; 21(6):923-9.
- 19. Mancia G., Fagard R., Narkiewicz K., et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J. Hypertens. 2013; 31(7):1281-357.
- 20. Malinski M.K., Skelton T.N., Leggett S.B., et al. Alcohol and blood pressure: a meta- analysis of dose-response relationships. Am J Epidemiol. 1993; 138(8):621-8.
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
Conflicts of Interest
No conflicts of interest in this work.
About this article
Cite this article
Shashibhushan J., Venkatesh V. Madholli et al., Risk Factors, Clinical Profile, Outcome in Hypertensive Crisis. Jr. Med. & Health Sci. 2024;11(2):47–58
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| October 21, 2024 | November 22, 2024 | December 30, 2024 |
DOI: https://doi.org/10.21088/ijmhs.2347.9981.11224.1
Keywords
Hypertensive crisiscerebrovascular accidenthypertensionsmokingECG abnormalitiescerebrovascular accidenthypertensionsmokingECG abnormalitiesSearch for Similar Articles
Similar Articles
- Wound Assessment using a Smartphone-based Application: Imitomeasure in Pressure...
- Emerging Pandemic and Silent Killer – Non Aloholic Fatty Liver Disease: A Compr...
- Prenatal and Postnatal Healthcare in Odisha
- Assessment of Diabetic Foot Ulcers: A Review
- IBS – Irritable Bowel Syndrome – Management through Comprehensive Non-Pharmacolo...
Article Level Metrics
Last UpdatedWednesday 08 July 2026, 09:07:45 (IST)
756
Accesses
6
309
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | October 21, 2024 |
| Accepted | November 22, 2024 |
| Published | December 30, 2024 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.