Full Text (PDF)
Indian Journal of Emergency Medicine 8(1):p 27-29, January–March 2022. | DOI: https://doi.org/10.21088/ijem.2395.311X.8122.4
Case Report
An Atypical Presentation of Acute Coronary Syndrome
Sudip Chakraborty, Debanjana Mukherjee, Souvik Goswami
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator
Indian Journal of Emergency Medicine 8(1):p 27-29, January–March 2022. | DOI: https://doi.org/10.21088/ijem.2395.311X.8122.4
How Cite This Article:
Sudip Chakraborty, Debanjana Mukherjee, Souvik Goswami/ An Atypical Presentation of Acute Coronary Syndrome/Indian J Emerg Med 2022;8(1):27–29.Timeline
Received : December 23, 2021
Accepted : February 12, 2022
Published : March 30, 2022
Abstract
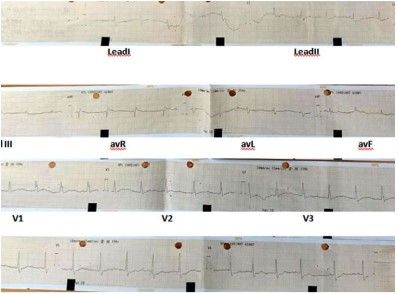
A 62 year old male patient was presented in ER due to the sudden onset of a precordial chest pain for an hour which aggravated in the last 30 minutes along with vomiting. The patient had no medical co-morbidities as such but had a known case of haemorrhoids and was a chronic smoker. On admission, he was conscious about the time and place and his vitals were HR: 50, BP: 110/70 mm of hg, RR: 20/min, SPO2: 99% (RA), CBG: 163 mg/dl. We could not find any evidence of MI in ECG, or any wall motion abnormality in ECHO but the patient was still complaining of chest pain and diaphoresis even post getting treated with isosorbide dinitrate and ranolazine. So, we took the patient to the Cath lab for a coronary angiography, which revealed LCX proximal 95-99% disease and RCA minor plaque in mid-part and diffuse disease in distal RCA. Primary PCI to LCX was done and treated conservatively. From this particular case, we learnt the significance of coronary angiography in ACS even if there was no significant finding on ECG, ECHO or cardiac enzymes. Message: Coronary Angiography played a major role to rule out acute coronary syndrome even though there was no change in ECG, cardiac markers and 2D-Echocardiography.
References
- 1. The Pharmaceutical Journal, 2015. Acute coronary syndrome guideline.
- 2. Hirachan, A., 2021. Rare Case of Dual Right Coronary Artery Intervention Presenting asAcute Coronary Syndrome. Clinical Cardiology and Cardiovascular Interventions, 04(16),pp.01-03.
- 3. Trost, J. and Lange, R., 2011. Treatment of acute coronary syndrome: Part 1: Non-ST-segment acute coronary syndrome. Critical Care Medicine, 39(10),pp.2346-2353.
- 4. Inami, S., Takano, M. and Mizuno, K., 2012. Acute Coronary Syndrome: Insights Based on Intravascular Imaging. Journal of the Japanese Coronary Association, 18(2),pp.107-117.
- 5. Chaowalit, N., Yipintsoi, T., Tresukosol, D., Kanjanavanit, R., Kiatchoosakun, S. and Representing the Thai Acute Coronary Syndrome Registry, 2009. Prognostic Value of Selected Presenting Features of Acute Coronary Syndrome in Predicting In-Hospital Adverse Events: Insight from the Thai Acute Coronary Syndrome Registry. Internal Medicine, 48(9),pp.639-646.
- 6. Millsaps, R., 1989. Echocardiogram Profiles After Acute Myocardial Infarction. Critical Care Medicine, 17(5),p.487.
- 7. Yavagal, S. and Baliga, V., 2019. Non-ischemic regional wall motion abnormality. Journal of The Indian Academy of Echocardiography & Cardiovascular Imaging, 3(1),p.7.
- 8. Yavagal, S. and Baliga, V., 2019. Non-ischemic regional wall motion abnormality. Journal of The Indian Academy of Echocardiography & Cardiovascular Imaging, 3(1),p.7.
- 9. azeem, s., 2018. Accuracy of 12 lead ECG for diagnosis of posterior myocardial infarction taking 15 lead ECG as gold standard. Journal of Medical Biomedical And Applied Sciences,6(9).
- 10. ŞAHİN, M., GÖRMELİ, C., DAĞ, N. and KURT, F., 2021.Comparison of multi-detector computed tomography coronary angiography with invasive coronary angiography in patients with coronary artery disease. MedicalRecords
- 11. Soiza, R., Leslie, S., Harrild, K., Peden, N. and Hargreaves, A., 2005. Age-Dependent Differences in Presentation, Risk Factor Profile, and Outcome of Suspected Acute Coronary Syndrome. Journal of the American Geriatrics Society, 53(11),pp.1961-1965.
- 12. The Pharmaceutical Journal, 2020. Acute coronary syndrome: risk factors, diagnosis and treatment.
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
Conflicts of Interest
No conflicts of interest in this work.
About this article
Cite this article
Sudip Chakraborty, Debanjana Mukherjee, Souvik Goswami/ An Atypical Presentation of Acute Coronary Syndrome/Indian J Emerg Med 2022;8(1):27–29.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator
| Received | Accepted | Published |
|---|---|---|
| December 23, 2021 | February 12, 2022 | March 30, 2022 |
DOI: https://doi.org/10.21088/ijem.2395.311X.8122.4
Keywords
Acute coronary syndromeCoronary angiographyChest painNo regional wall motion abnormalityECGSearch for Similar Articles
Similar Articles
- Covid 19 Vaccine: Associated Henoch Schonlein Purpura in Young Adult Female
- A Rare Case of Intolerance to Medically Approved Dose of Sildenafil Citrate in a...
- Acute Mesenteric Ischemia: An Unusual Cause of Hematemesis in a 48 Year Old Man
- Brachial Artery Pseudoaneurysm Related Causally to Iatrogenic Coagulopathy in a...
- Combination Therapy for Acute Management of Yellow Oleander Poisoning: A Case Re...
Article Level Metrics
Last UpdatedTuesday 07 July 2026, 11:36:50 (IST)
2530
Accesses
5
890
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | December 23, 2021 |
| Accepted | February 12, 2022 |
| Published | March 30, 2022 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator