Full Text (PDF)
Indian Journal of Anesthesia and Analgesia 11(3):p 155-157, July- September 2024. | DOI: https://doi.org/10.21088/ijaa.2349.8471.11324.8
Case Report
Airway and Anaesthetic Management of Massive Ameloblastoma with Free Fibular Graft and Osteocutaneous Flap
Susmitha Thummala, Ravi Madhusudhana
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Anesthesia and Analgesia 11(3):p 155-157, July- September 2024. | DOI: https://doi.org/10.21088/ijaa.2349.8471.11324.8
How Cite This Article:
Thummala S, Madhusudhana R. Airway and anaesthetic management of massive ameloblastoma with free fibular graft and osteocutaneous flap. Ind J Anesth Analg. 2024;11(3):155-7.Timeline
Received : March 30, 2024
Accepted : September 27, 2024
Published : September 28, 2024
Abstract
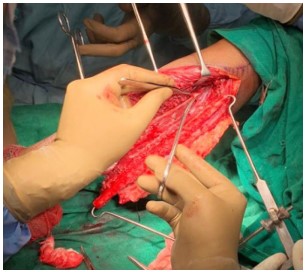
Introduction: Intubation can sometimes be difficult in patients with lesions in the mouth floor. Ameloblastoma is a frequently encountered tumor of the maxillofacial area. An extensive lesion might occupy the floor of the mouth, prevent displacement of the tongue, limiting the space for inserting a laryngoscope blade and resulting in difficult intubation even with fiberoptic bronchoscopy. Ameloblastoma is a common neoplasm affecting the jaws. It is an aggressive benign tumor of epithelial origin. Ameloblastomas are recognized for their invasive growth and tendency to recur. Reconstruction procedures are usually prolonged and require meticulous attention to fluid replacement, blood loss and prevention of hypothermia. Hence they present a challenge to the anaesthesiologist. Case Report: A 40-year-old woman weighing 36 kgs presented with pain and swelling in the right jaw/mandible that had existed for three years. Her past medical history was unremarkable. Upon airway examination, mouth opening was inadequate, restriction of head and neck movements was noted, CECT showed pneumocysts in C5, C6 and C7 vertebrae and showed a large expansile lytic lesion involving body of mandible and inferior aspect of rami bilaterally with cysts and solid components show heterogeneous post contrast enhancement with mass effect on adjacent structures. The results of general and systemic examination were within normal limits. Two large bore 16G cannulas secured for proper fluid resuscitation intraoperatively, as mouth opening is inadequate and difficult bag and mask ventilation anticipated. Planned for awake fibreoptic intubation, patient premedicated with Glycopyrrolate and Fentanyl. As expected patient had breathing difficulty during the procedure and laryngeal edema seen on fibreoptic, patient given Dexamethasone 8mg, preoxygenated with facemask for 10 minutes and opted for 6mm ID flexometallic ET tube fibreoptic intubation. Torniquet applied for 2 hours to left thigh to minimize blood loss for fibular graft patient developed hypotension after 8 hours of surgery PRBC and colloids transfused and resuscitated with fluids as surgeons opted for tracheostomy in between, after 16 hours of surgery patient shifted to ICU for observation shifted back to ward. Conclusion: Our case was anticipated difficult airway, planned for awake fibreoptic intubation,even though it was prepared, because of the tumor, airway edema present and all small size endo tracheal tube was used surgical airway was ruled out as tumor was big and was in midline.
References
- 1. Dureja J, Balhara S, Saini S, Ghai A. Airway Management in Ameloblastoma- A Case Report. J Anaesth Clin Pharmacol 2005; 21(3): 317-19.
- 2. Kalavrezos N, Baldwin DJ, Walker DM. Giant neglected ameloblastoma: Single stage treatment and clinicopathological review. Br J Oral Maxillofac Surg 2008;46:591-3.
- 3. Adekeye EO, McLavery K. Recurrent ameloblastoma of the maxillofacial region. Clinical features and treatment. J Maxillofac Surg 1986; 14:153-7.
- 4. Scholar Iohom G, Ronayne M, Cunningham AJ. Prediction of difficult tracheal intubation. Eur J Anaesthesiol. 2003;20:31–36.
Data Sharing Statement
There are no additional data available.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
Information not provided.
Conflicts of Interest
The authors report no conflicts of interest in this work.
About this article
Cite this article
Thummala S, Madhusudhana R. Airway and anaesthetic management of massive ameloblastoma with free fibular graft and osteocutaneous flap. Ind J Anesth Analg. 2024;11(3):155-7.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| March 30, 2024 | September 27, 2024 | September 28, 2024 |
DOI: https://doi.org/10.21088/ijaa.2349.8471.11324.8
Keywords
Difficult AirwayAmeloblastoma of MandibleFibreoptic IntubationSearch for Similar Articles
Similar Articles
- Awake Fibreoptic Intubation for Airway Management in Massive Thyroid Enlargement...
- A Case of Thoracotomy with One Lung Ventilation for Carcinoma Oesophagus
- A Case of Empyema for Thoracotomy and Decortication-Anaesthesia Management
- Full Mouth Rehabilitation in a 3-Year-Old Female Child with Repaired Tetralogy o...
- Do Gel Manicures Affect SpO2 Readings ? A Clinical Investigation
Article Level Metrics
Last UpdatedMonday 13 July 2026, 19:00:00 (IST)
5660
Accesses
9
679
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | March 30, 2024 |
| Accepted | September 27, 2024 |
| Published | September 28, 2024 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.