Full Text (PDF)
Indian Journal of Emergency Medicine 11(4):p 227-231, Oct - Dec. 2025. | DOI: https://doi.org/10.21088/ijem.2395.311X.11425.3
Case Report
Rare Wellen’s Rare Presentation
Unnati Singh, Rijul Bhatia, Anita Rawat, Kishalay Datta
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Emergency Medicine 11(4):p 227-231, Oct - Dec. 2025. | DOI: https://doi.org/10.21088/ijem.2395.311X.11425.3
How Cite This Article:
Singh U, Bhatia R, Rawat A, et al. Rare Wellen’s Rare Presentation. Ind J Emerg Med. 2025; 11(4): 227-231.Timeline
Received : May 21, 2025
Accepted : June 30, 2025
Published : December 30, 2025
Abstract
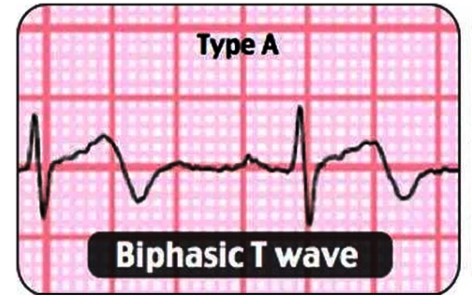
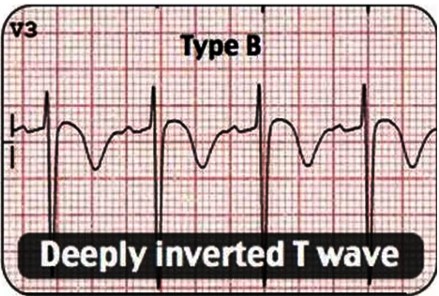
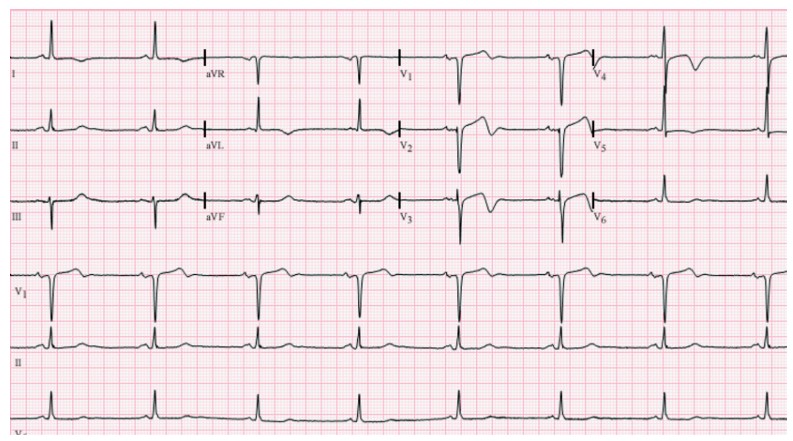
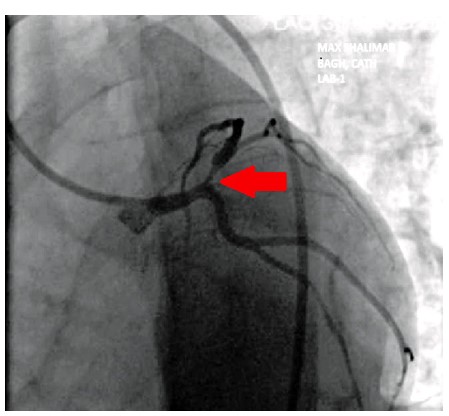
Wellens syndrome is a distinct electrocardiographic (ECG) finding that reflects critical narrowing of the proximal left anterior descending (LAD) coronary artery. First identified in 1982, this pattern typically appears in patients with a history of unstable angina, especially during pain-free intervals. Recognizing this syndrome is vital, as it signals a high risk for imminent anterior wall myocardial infarction if not treated promptly. The syndrome is classified into two types based on T wave morphology. Type A, which features biphasic T waves most prominently in leads V2 and V3, can be particularly challenging to identify. These subtle ECG changes are often overlooked, especially when the patient is not actively experiencing chest pain, which increases the risk of misdiagnosis or delayed treatment. Such oversight can lead to rapid deterioration and serious cardiac complications, including extensive myocardial infarction. In this case report, we present a patient with type A Wellens syndrome, where the early ECG showed only mild biphasic T wave abnormalities that were initially missed. This diagnostic oversight delayed appropriate cardiologic intervention and emphasized the importance of vigilance in evaluating atypical or transient ECG changes. Early identification of Wellens syndrome, even in asymptomatic phases, is critical to guiding appropriate management and preventing life-threatening outcomes. Clinicians, particularly in emergency medicine settings, should be aware of these subtle yet significant ECG markers.
References
- 1. de Zwaan C., Bär FWHM, Wellens HJJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982; 103(4): 730–6. https://doi.org/10.1016/00028703(82)90480-X
- 2. Tandy T.K., Bottomy D.P., Lewis J.G. Wellens’ syndrome. Ann Emerg Med. 1999; 33(3): 347–51. https://doi.org/10.1016/S01960644(99)70373-2
- 3. de Zwaan C., Bär FW, Janssen JHA, Cheriex E.C., Dassen WRM, Brugada P., et al. Angiographic and clinical characteristics of patients with unstable angina showing an ECG pattern indicating critical narrowing of the proximal LAD coronary artery. Am Heart J. 1989; 117(3): 657–65. https://doi.org/10.1016/0002-8703(89)90742-4.
- 4. Kobayashi A., Misumida N., Kanei Y., Fox J. CRT-111 prevalence and prognostic value of Wellens’ sign in patients with non-ST elevation myocardial infarction. JACC Cardiovasc Interv. 2015; 8(2 Suppl): S11–2. https://doi.org/10.1016/j.jcin.2014.12.041
- 5. Rhinehardt J., Brady W.J., Perron A.D., Mattu A. Electrocardiographic manifestations of Wellens’ syndrome. Am J Emerg Med. 2002; 20(7): 638–43. https://doi.org/10.1053/ajem.2002.34800
- 6. Oo SZMWH, Khalighi K., Kodali A., May C., Aung T.T., Snyder R. Ominous T-wave inversions: Wellens’ syndrome revisited. J Community Hosp Intern Med Perspect. 2016; 6(4). https://doi.org/10.3402/jchimp.v6.32011
- 7. Grautoff S. Wellens’ syndrome can indicate high-grade LAD stenosis in case of left bundle branch block. Herzschrittmacherther Elektrophysiol. 2017; 28(1): 57–9. https://doi.org/10.1007/s00399-017-0489-z
- 8. Hsu Y.C., Hsu C.W., Chen T.C. Type B. Wellens’ syndrome: electrocardiogram patterns that clinicians should be aware of. Tzu Chi Med J. 2017; 29(2): 127–8. https://doi.org/10.4103/tcmj.tcmj_26_17
- 9. Sedhai Y.R., Pawar A.S., Bhattacharya P.T., Basnyat S. Wellens’ syndrome, a case report of an electrocardiographic warning sign. J Adv Intern Med. 2017; 5(1): 19–23. https://doi.org/10.3126/jaim.v5i1.17067
- 10. Inayat F., Riaz I., Ali N.S., Figueredo V.M. Pseudo-Wellens’ syndrome secondary to concurrent cannabis and phencyclidine intoxication. BMJ Case Rep. 2018. https://doi. org/10.1136/bcr-2018-225755
- 11. Migliore F., Zorzi A., Perazzolo Marra M., Iliceto S., Corrado D. Myocardial edema as a substrate of electrocardiographic abnormalities and life-threatening arrhythmias in reversible ventricular dysfunction of Takotsubo cardiomyopathy: imaging evidence, presumed mechanisms, and implications for therapy. Heart Rhythm. 2015; 12(8): 1867–77. https:/doi.org/10.1016/j.hrthm.2015.04.041
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
Conflicts of Interest
No conflicts of interest in this work.
About this article
Cite this article
Singh U, Bhatia R, Rawat A, et al. Rare Wellen’s Rare Presentation. Ind J Emerg Med. 2025; 11(4): 227-231.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| May 21, 2025 | June 30, 2025 | December 30, 2025 |
DOI: https://doi.org/10.21088/ijem.2395.311X.11425.3
Keywords
Wellens syndromeMyocardial infarctionVigilanceAbnormalitiesSearch for Similar Articles
Similar Articles
- Covid 19 Vaccine: Associated Henoch Schonlein Purpura in Young Adult Female
- A Rare Case of Intolerance to Medically Approved Dose of Sildenafil Citrate in a...
- Acute Mesenteric Ischemia: An Unusual Cause of Hematemesis in a 48 Year Old Man
- Brachial Artery Pseudoaneurysm Related Causally to Iatrogenic Coagulopathy in a...
- Combination Therapy for Acute Management of Yellow Oleander Poisoning: A Case Re...
Article Level Metrics
Last UpdatedTuesday 28 July 2026, 04:05:59 (IST)
3277
Accesses
15
910
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | May 21, 2025 |
| Accepted | June 30, 2025 |
| Published | December 30, 2025 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.