Full Text (PDF)
Indian Journal of Emergency Medicine 11(4):p 283-288, Oct - Dec. 2025. | DOI: https://doi.org/10.21088/ijem.2395.311X.11425.13
Case Report
A Rare Case of Hypercoagulable State Due to Combined Inherited Thrombophilia Protein C & S Deficiency and Possible Anti Phospholipid Syndrome Complicated by a Pulmonary Embolism Causing Cardiac Strain
Paayal Bhattacharya, Anoop Purkayastha
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Emergency Medicine 11(4):p 283-288, Oct - Dec. 2025. | DOI: https://doi.org/10.21088/ijem.2395.311X.11425.13
How Cite This Article:
Bhattacharya P, Purkayastha A. A Rare Case of Hypercoagulable State Due to Combined Inherited Thrombophilia Protein C & S Deficiency and Possible Anti Phospholipid Syndrome Complicated by a Pulmonary Embolism Causing Cardiac Strain. Ind J Emerg Med. 2025;11(4):283-8.Timeline
Received : April 28, 2025
Accepted : June 17, 2025
Published : December 30, 2025
Abstract
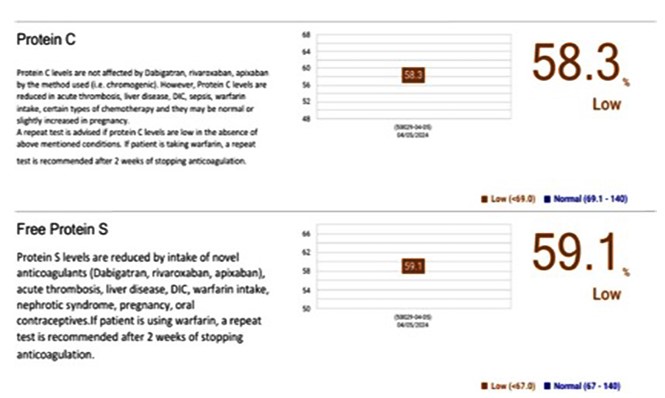
This is case report of a 31 year old male patient who came to emergency department with complaints of sudden onset shortness of breath associated with cardinal signs of cardiac strain followed on to be diagnosed with combined inherited thrombophilia due to protein S and protein C deficiency along with a possible antiphospholipid syndrome (APS). The case was complicated by pulmonary embolism with cardiac strain as indicated by grossly elevated NT-ProBNP and 2D Echo changes like global LV Hypokinesia and PASP of 60mmHg
References
- 1. De Stefano V., Leone G., Mastrangelo S., Tripodi A., Rodeghiero F., Castaman G., Barbui T., Finazzi G., Bizzi B., Mannucci P.M. Clinical manifestations and management of inherited thrombophilia: retrospective analysis and follow-up after diagnosis of 238 patients with congenital deficiency of antithrombin III, protein C, protein S. Thrombosis and haemostasis. 1994; 72(09): 352-8.
- 2. Nesbitt G.C., Mankad S., Oh J.K. Strain imaging in echocardiography: methods and clinical applications. The international journal of cardiovascular imaging. 2009 Apr; 25: 9-22.
- 3. Piazza G. Thrombophilia and Hypercoagulability. Circulation. 2014 Jul 8; 130(2): e9-10.
- 4. Previtali E., Bucciarelli P., Passamonti S.M., Martinelli I. Risk factors for venous and arterial thrombosis. Blood transfusion. 2011 Apr; 9(2): 120.
- 5. Egeberg O. Inherited antithrombin deficiency causing thrombophilia. Thrombosis and Haemostasis. 1965; 13(02): 516-30.
- 6. Griffin J.H., Evatt B.R., Zimmerman T.S., Kleiss A.J., Wideman C. Deficiency of protein C in congenital thrombotic disease. The Journal of clinical investigation. 1981 Nov 1; 68(5): 1370-3.
- 7. Comp P.C., Esmon C.T. Recurrent venous thromboembolism in patients with a partial deficiency of protein S. New England Journal of Medicine. 1984 Dec 13; 311(24): 1525-8.
- 8. Moosazadeh M., Espahbodi F., Afshari M., Eslami A. Can CBC Profile and Liver Function Test Predict Chronic Kidney Disease among a Normal Population?. International journal of preventive medicine. 2023 Jan 1; 14(1): 2.
- 9. Siennicka A., Kłysz M., Chełstowski K., Tabaczniuk A, Marcinowska Z., Tarnowska P, Kulesza J., Torbe A., Jastrzębska M. Reference Values of D-Dimers and Fibrinogen in the Course of Physiological Pregnancy: the Potential Impact of Selected Risk Factors—A Pilot Study. BioMed research international. 2020; 2020(1): 3192350.
- 10. Nakashima M.O., Rogers H.J. Hypercoagulable states: an algorithmic approach to laboratory testing and update on monitoring of direct oral anticoagulants. Blood research. 2014 Jun 25; 49(2): 85.
- 11. Goldhaber S.Z., Agnelli G., Levine M.N. Reduced dose bolus alteplase vs conventional alteplase infusion for pulmonary embolism thrombolysis: an international multicenter randomized trial. Chest. 1994 Sep 1; 106(3): 718-24.
- 12. Maizel A.S., Bookstein J.J. Streptokinase, urokinase, and tissue plasminogen activator: pharmacokinetics, relative advantages, and methods for maximizing rates and consistency of lysis. Cardiovascular and interventional radiology. 1986 Sep; 9: 236-44.
- 13. Hadj A.K., Nikfarjam M. Post-procedural considerations. In Principles of Flexible Endoscopy for Surgeons 2013 Mar 27 (pp. 5562). New York, NY: Springer New York.
- 14. Josephson M.E., Callans D.J. Using the twelvelead electrocardiogram to localize the site of origin of ventricular tachycardia. Heart Rhythm. 2005 Apr 1; 2(4): 443-6.
- 15. Kumar U.D., Nareppa U., Shetty S.P., Wali M. Right ventricular thrombus in case of atrial septal defect with massive pulmonary embolism: a diagnostic dilemma. Annals of Cardiac Anaesthesia. 2016 Jan 1; 19(1): 173-6.
- 16. Lameire N., Adam A., Becker C.R., Davidson C., McCullough P.A., Stacul F., Tumlin J., Panel C.C. Baseline renal function screening. The American journal of cardiology. 2006 Sep 18; 98(6): 21-6.
- 17. Majid Z., Tahir F., Arif T.B., Ahmed J. Chronic non-cirrhotic portal vein thrombosis with cavernous transformation secondary to protein c and s deficiency. Cureus. 2020 Feb 29; 12(2).
- 18. Ueno N., Sasaki A., Tomiyama T., Tano S., Kimura K. Color Doppler ultrasonography in the diagnosis of cavernous transformation of the portal vein. Journal of clinical ultrasound. 1997 Jun; 25(5): 227-33.
- 19. Rodríguez-Leal G.A., Morán S., Corona-Cedillo R, Brom-Valladares R. Portal vein thrombosis with protein CS deficiency in a non-cirrhotic patient. World Journal of Hepatology. 2014 Jul 27; 6(7): 532.
- 20. Denninger M.H., Chaït Y., Casadevall N., Hillaire S., Guillin M.C., Bezeaud A., Erlinger S., Briere J., Valla D. Cause of portal or hepatic venous thrombosis in adults: The role of multiple concurrent factors. Hepatology. 2000 Mar; 31(3): 587-91.
- 21. Fisher N.C., Wilde J.T., Roper J., Elias E. Deficiency of natural anticoagulant proteins C., S., and antithrombin in portal vein thrombosis: a secondary phenomenon? Gut. 2000 Apr 1; 46(4): 534-9
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
Conflicts of Interest
No conflicts of interest in this work.
About this article
Cite this article
Bhattacharya P, Purkayastha A. A Rare Case of Hypercoagulable State Due to Combined Inherited Thrombophilia Protein C & S Deficiency and Possible Anti Phospholipid Syndrome Complicated by a Pulmonary Embolism Causing Cardiac Strain. Ind J Emerg Med. 2025;11(4):283-8.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| April 28, 2025 | June 17, 2025 | December 30, 2025 |
DOI: https://doi.org/10.21088/ijem.2395.311X.11425.13
Keywords
Hypercoagulable stateProtein C deficiency• Hypercoagulable state • Protein C deficiency • Protein S deficiency • InheritedProtein S deficiencyInherited thrombophiliaAntiphospholipid syndrome (APS)Pulmonary embolismCardiac strainSearch for Similar Articles
Similar Articles
- Covid 19 Vaccine: Associated Henoch Schonlein Purpura in Young Adult Female
- A Rare Case of Intolerance to Medically Approved Dose of Sildenafil Citrate in a...
- Acute Mesenteric Ischemia: An Unusual Cause of Hematemesis in a 48 Year Old Man
- Brachial Artery Pseudoaneurysm Related Causally to Iatrogenic Coagulopathy in a...
- Combination Therapy for Acute Management of Yellow Oleander Poisoning: A Case Re...
Article Level Metrics
Last UpdatedSunday 26 July 2026, 17:39:56 (IST)
3245
Accesses
23
910
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | April 28, 2025 |
| Accepted | June 17, 2025 |
| Published | December 30, 2025 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.