Full Text (PDF)
Indian Journal of Obstetrics and Gynecology 12(4):p 167-174, October-December 2024. | DOI: https://doi.org/10.21088/ijog.2321.1636.12424.4
Case Report
Management of Placenta Accreta Spectrum Cases (PAS) by Uterine Artery Emobolisation: A Hybrid Approach
Shripad Hebbar, Rajani Upadhyaya, Bhawna Singhal, Kavisha Bhat, Divyashree Bhat
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Obstetrics and Gynecology 12(4):p 167-174, October-December 2024. | DOI: https://doi.org/10.21088/ijog.2321.1636.12424.4
How Cite This Article:
Rajani Upadhyaya, Bhawna Singhal, Shripad Hebbar et al. Management of Placenta Accreta Spectrum Cases (PAS) by Uterine Artery Emobolisation: A Hybrid Approach. Indian J Obstet Gynecol. 2024;12(4):167-174.Timeline
Received : November 18, 2024
Accepted : December 27, 2024
Published : December 30, 2024
Abstract
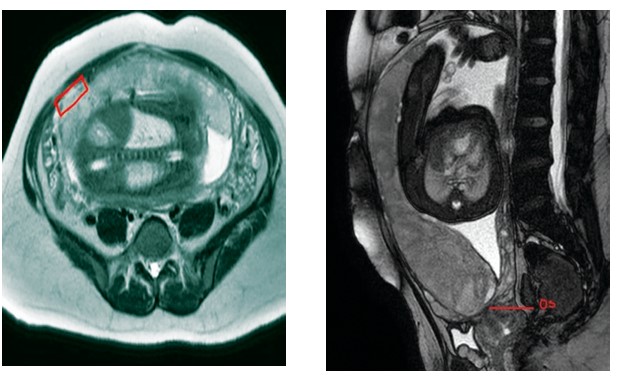
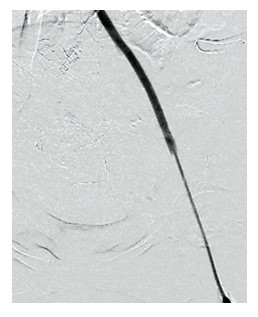
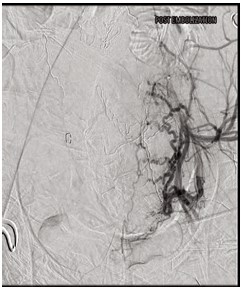
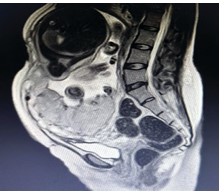
Background: Conservative methods for the management of placenta accreta spectrum disorders includes all the methods which aims to reduce the morbidity associated with peripartum hysterectomy, intraoperative complications, blood loss during surgery and mainly to preserve future fertility. These methods are to be practiced as much as possible in appropriate cases after weighing risks and benefits. Objective: To report two cases of placenta accreta which were managed by uterine artery embolization followed by caesarean section in a hybrid operation theatre in our tertiary care centre. Cases: This is a case series of two cases of pregnant women who were diagnosed to be having placenta accreta spectrum disorder. Here, we describe the steps and outcomes of the above-mentioned method. Conclusion: Uterine artery embolization prior to caesarean section in selected cases of placenta accreta spectrum disorders is a feasible and advantageous procedure. It decreases the operating time, intraoperative blood loss and complications, and ICU stay. Larger studies may be needed to confirm the advantages.
References
- 1. Y. Oyelese and J. C. Smulian, “Placenta previa, placenta accreta, and vasa previa,” Obstetrics and Gynecology, vol. 107, no. 4, pp. 927–941, 2006.
- 2. Sentilhes, L.; Ambroselli, C.; Kayem, G.; Provansal, M.; Fernandez, H.; Perrotin, F.; Winer, N.; Pierre, F.; Benachi, A.; Dreyfus, M. Maternal outcome after conservative treatment of placenta accreta. Obstet. Gynecol. 2010, 115, 526–534.
- 3. Kayem, G.; Davy, C.; Goffinet, F.; Thomas, C.; Clément, D.; Cabrol, D. Conservative versus extirpative management in cases of placenta accreta. Obstet. Gynecol. 2004, 104, 531–536.
- 4. Oyelese Y, Smulian JC. Placenta previa, et al. 2006. Obstet Gynecol. 107: 927-41.
- 5. Binkowska M, Ciebiera M, Jakiel G. Placenta accreta: Review and 3 case reports. Ginekol Pol. 2015; 86(5):396400.
- 6. Miller DA, Chollet JA, Goodwin TM. 1997. Clinical risk factors for placenta previa-placenta accreta. Am J Obstet Gynecol. 177: 210-214.
- 7. Cunningham, F.G.; Leveno, K.J.; Bloom, S.L.; Dashe, J.S.; Hoffman, B.L.; Casey, B.M.; Spong, C.Y. Obstetrical Hemorrhage. In Williams Obstetrics, 25th ed.; McGraw-Hill Education: New York, NY, USA, 2018.
- 8. Bailit, J.L.; Grobman, W.A.; Rice, M.M.; Reddy, U.M.; Wapner, R.J.; Varner, M.W.; Leveno, K.J.; Iams, J.D.; Tita, A.T.N.; Saade, G.; et al. Morbidly adherent placenta treatments and outcomes. Obstet. Gynecol. 2015, 125, 683–689.
- 9. El Gelany, S.; Mosbeh, M.H.; Ibrahim, E.M.; Mohammed, M.; Khalifa, E.M.; Abdelhakium, A.K.; Yousef, A.M.; Hassan, H.; Goma, K.; Alghany, A.A.; et al. Placenta Accreta Spectrum (PAS) disorders: Incidence, risk factors and outcomes of different management strategies in a tertiary referral hospital in Minia, Egypt: A prospective study. BMC Pregnancy Childbirth 2019, 19, 313.
- 10. Tikkanen M, Paavonen J, Loukovaara M, Stefanovic V. Antenatal diagnosis of placenta accreta leads to reduced blood loss. ActaObstetGynecol Scand. 2011;90:1140–1146.
- 11. Wong HS, Cheung YK, Zuccollo J, Tait J, Pringle KC. Evaluation of sonographic diagnostic criteria for placenta accreta. J Clin Ultrasound 2008; 9: 551– 559.
- 12. S. L. Collins, A. Ashcroft, T. Braun, P. Calda, J. Langhoff-Roos, O. Morel, V. Stefanovic, B. Tutschek, F. Chantraine, on behalf of the European Working Group on Abnormally Invasive Placenta (EW-AIP), First published: 21 July 2015 https://doi. org/10.1002/uog.14952.
- 13. Downes, K.L.; Hinkle, S.N.; Sjaarda, L.A.; Albert, P.S.; Grantz, K.L. Previous prelabor or intrapartumcesarean delivery and risk of placenta previa. Am. J. Obstet. Gynecol. 2015, 212, e1–e6.
- 14. AngstmannT,Gard G, Harrington T, Ward E, Thomson A, Giles W. Surgical management of placenta accreta: a cohort series and suggested approach. Am J ObstetGynecol2010; 202: 38.e1 – 9.
- 15. Gyamfi-Bannerman C. Society for Maternal Fetal Medicine (SMFM) Consult Series #44: management of bleeding in the late preterm period. Society for Maternal-Fetal Medicine (SMFM). Am J ObstetGynecol2018 ; 218 : B2 – 8.
- 16. Sentilhes L, Kayem G, Chandraharan E, Palacios Jaraquemada J, Jauniaux E. FIGO consensus guidelines on placenta accreta spectrum disorders: Conservative management. Int J Gynecol Obstet. 2018;140:291–298.
- 17. Fox KA,Shamshirsaz AA, Carusi D, Secord AA, Lee P, Turan OM, et al. Conservative management of morbidly adherent placenta: expert review. Am J ObstetGynecol2015; 213 : 755 – 60.
- 18. Perez-DelboyA, Wright JD. Surgical management of placenta accreta: to leave or remove the placenta? BJOG 2014 ; 121: 163 – 9;
- 19. Agostini A, Vejux N, Bretelle F, Collette E, De Lapparent T, Cravello L, et al. Value of laparoscopic assistance for vaginal hysterectomy with prophylactic bilateral oophorectomy. Am J ObstetGynecol2006 ; 194 : 351 – 4.
- 20. Legro RS, Price FV, Hill LM, Caritis SN. Nonsurgical management of placenta percreta: A case report. Obstet Gynecol. 1994; 83(5 Pt 2):847-9.
- 21. Butt K, Gagnon A, Delisle MF. Failure of methotrexate and internal iliac balloon catheterization to manage placenta percreta. Obstet Gynecol. 2002; 99(6):981-2.
- 22. Pan Y., Zhou X., Yang Z., Cui S., De W., Sun L. Retrospective cohort study of prophylactic intraoperative uterine artery embolization for abnormally invasive placenta. Int. J. Gynaecol. Obstet. 2017;137:45–50. doi: 10.1002/ijgo.12090.
- 23. Paull J.D., Smith J., Williams L., Davison G., Devine T., Holt M. Balloon occlusion of the abdominal aorta during caesarean hysterectomy for placenta percreta. Anaesth. Intensive Care. 1995;23:731–734.
- 24. Dubois J., Garel L., Grignon A., Lemay M., Leduc L. Placenta percreta: Balloon occlusion and embolization of the internal iliac arteries to reduce intraoperative blood losses. Am. J. Obstet. Gynecol. 1997;176:723–726. doi: 10.1016/ S0002-9378(97)70582-9.
- 25. Huang KL, Tsai CC, Fu HC, Cheng HH, Lai YJ, Hung HN, Tsang LL, Hsu TY. Prophylactic Transcatheter Arterial Embolization Helps Intraoperative Hemorrhagic Control for Removing Invasive Placenta. J Clin Med. 2018 Nov 21;7(11):460. doi: 10.3390/jcm7110460. PMID: 30469429; PMCID: PMC6262565.
- 26. Cottier, J.; Fignon, A.; Tranquart, F.; Herbreteau, D. Uterine necrosis after arterial embolization for postpartum hemorrhage. Obstet. Gynecol. 2002, 100, 1074–1077.
- 27. Pan, Y.; Zhou, X.; Yang, Z.; Cui, S.; De, W.; Sun, L. Retrospective cohort study of prophylactic intraoperative uterine artery embolization for abnormally invasive placenta. Int. J. Gynecol. Obstet. 2017, 137, 45–50.
- 28. Mohan, B.; Wander, G.; Bansal, R.; Mutti, J.; Tandon, P.; Juneja, S.; Puri, S. Intra-operative uterine artery embolization with caesarean delivery in an adjoining operating theatre and catheter lab (OT/CL) complex vs. conventional management in patients with abnormally invasive placenta: A retrospective case control study. J. Obstet. Gynaecol. 2020, 40, 324–329.
- 29. Konishi, Y.; Yamamoto, S.; Sugiki, K.; Sakamoto, H.; Sawamura, S. A Novel and Multidisciplinary Strategy for Cesarean Delivery With Placenta Percreta: Intraoperative Embolization in a Hybrid Suite. AA Case Rep. 2016, 7, 135–138.
- 30. Meller, C.H.; Garcia-Monaco, R.D.; Izbizky, G.; Lamm, M.; Jaunarena, J.; Peralta, O.; Otaño, L. Non-conservative management of placenta accreta spectrum in the hybrid operating room: A retrospective cohort study. Cardiovasc. Intervent. Radiol. 2019, 42, 365–370.
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study
Conflicts of Interest
No conflicts of interest in this work
About this article
Cite this article
Rajani Upadhyaya, Bhawna Singhal, Shripad Hebbar et al. Management of Placenta Accreta Spectrum Cases (PAS) by Uterine Artery Emobolisation: A Hybrid Approach. Indian J Obstet Gynecol. 2024;12(4):167-174.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| November 18, 2024 | December 27, 2024 | December 30, 2024 |
DOI: https://doi.org/10.21088/ijog.2321.1636.12424.4
Keywords
Uterine artery embolizationConservative managementPlacenta accreta spectrum.Conservative managementPlacenta accreta spectrum.Search for Similar Articles
Similar Articles
- A Rare Case of Vaginal Vault Endometriosis in a Post Hysterectomised Woman: A Ca...
- An Incidental Dilemma of Degenerated Stony Parasitic Fibroid: A Rare Case Report
- Recurrence Ectopic Pregnancy in the Post Salpingectomy Stump: A Rare Case and Li...
- Obstetric Outcomes of Pregnancy with Uterine Fibroids
- Occupational Predictors of Obstetric and Perinatal Outcomes in Working Women in...
Article Level Metrics
Last UpdatedThursday 09 July 2026, 05:36:18 (IST)
1883
Accesses
8
349
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | November 18, 2024 |
| Accepted | December 27, 2024 |
| Published | December 30, 2024 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.