Full Text (PDF)
Indian Journal of Emergency Medicine 11(1):p 13-25, Jan -April 2025. | DOI: https://doi.org/10.21088/ijem.2395.311X.11125.2
Review Article
Bridging the Gap in Resuscitation Therapies: Centhaquine in Hypovolemic Shock
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Indian Journal of Emergency Medicine 11(1):p 13-25, Jan -April 2025. | DOI: https://doi.org/10.21088/ijem.2395.311X.11125.2
How Cite This Article:
Shah S. Bridging the gap in resuscitation therapies: centhaquine in hypovolemic shock. Ind J Emerg Med. 2025;11(1):13-25.Timeline
Received : January 11, 2025
Accepted : February 14, 2025
Published : April 20, 2025
Abstract
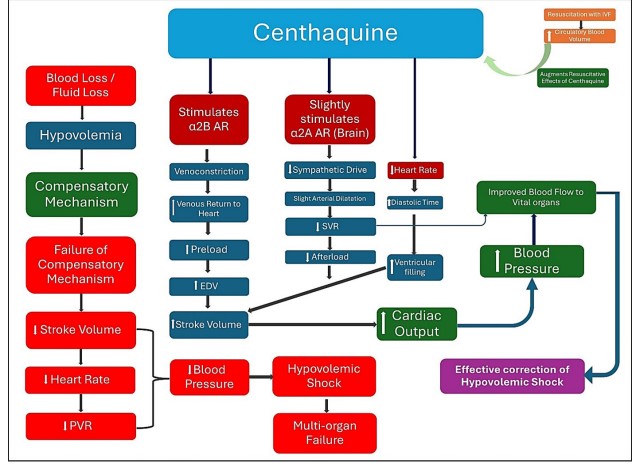
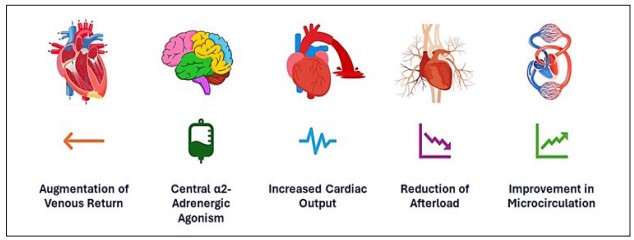
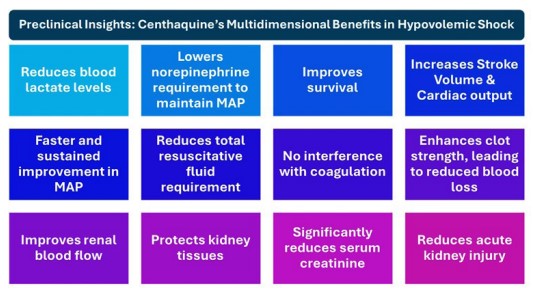
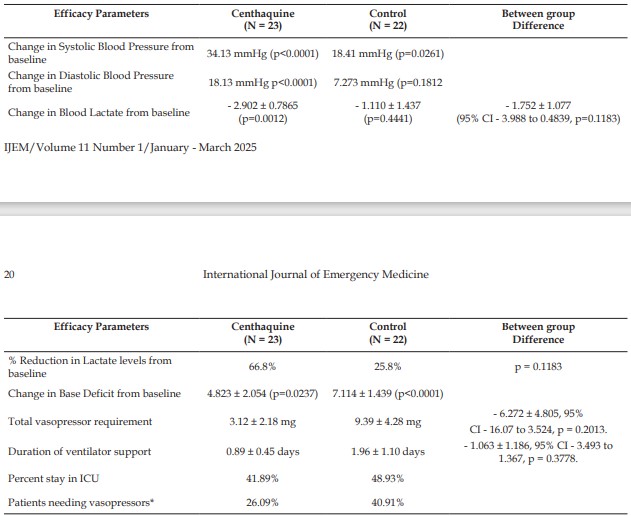
Hypovolemic shock is a life-threatening condition with high mortality, requiring urgent resuscitative therapy to restore perfusion and prevent irreversible organ damage alongside the definitive management. Current treatments, including fluid resuscitation with initially crystalloids and later blood or its components followed by vasopressors have certain limitations in effectively restoring hemodynamics and improving tissue perfusion besides some safety concerns. This review explores unique features of a novel first-in-class resuscitative agent centhaquine including unique mechanism of action, pure venoconstriction without arterial constriction and wide safety margin. The balanced modulation of venous return and arterial resistance allows centhaquine to increase cardiac output in patients with hypovolemic shock while maintaining the tissue perfusion without compromising microcirculatory flow, offering clinicians a more effective option to improve survival in these critically ill patients. Preclinical and clinical studies demonstrate that centhaquine significantly improves hemodynamic parameters, reduces vasopressor and fluid requirements, lowers blood lactate levels and improves survival in patients with hypovolemic shock. Centhaquine’s renoprotective effects further highlight its potential in preventing organ failure following hypovolemic shock. The safety profile of centhaquine has been established across multiple phases of clinical trials and it is currently approved in India for the treatment of hypovolemic shock. Centhaquine represents a promising advancement in the management of shock, offering a novel approach to improving patient outcomes. Further research could evaluate the potential of centhaquine in managing other forms of shock such as neurogenic shock and septic shock
References
- 1. Taghavi S., Askari R. Hypovolemic shock [Updated 2023 June 23]. In: StatPearls [Internet]. Treasure Island: StatPearls Publishing; 2021. https://www.ncbi.nlm.nih.gov/books/ NBK513297/.
- 2. Cannon J.W. Hemorrhagic shock. N. Engl J Med. 2018; 378(4): 370–379. doi: 10.1056/ NEJMra1705649.
- 3. Kaufman E.J., Richmond TS, Wiebe D.J., Jacoby S.F., Holena D.N. Patient experiences of trauma resuscitation. JAMA Surg. 2017; 152(9): 843–50. doi: 10.1001/jamasurg.2017.1088.
- 4. Gulati A., Choudhuri R., Gupta A., Singh S, Ali SKN, Sidhu GK, et al. A multicentric, randomized, controlled phase III study of centhaquine (Lyfaquin) as a resuscitative agent in hypovolemic shock patients. Drugs. 2021; 81(9): 1079-1100. doi: 10.1007/s40265- 021-01547-5.
- 5. Maier R.V. Pathogenesis of multiple organ dysfunction syndrome--endotoxin, inammatory cells, and their mediators: cytokines and reactive oxygen species. Surg Infect (Larchmt). 2000; 1(3): 197-204; discussion 204-5. doi: 10.1089/109629600750018123.
- 6. Khanna A., Vaidya K., Shah D., Ranjan A.K., Gulati A. Centhaquine increases stroke volume and cardiac output in patients with hypovolemic shock. Journal of Clinical Medicine. 2024; 13(13): 3765. https://doi. org/10.3390/jcm13133765.
- 7. Snyder E.M. Jr. Management of refractory shock. Calif. Med. 1954, 80(1), 13–15.
- 8. Kalkwarf K.J., Cotton B.A. Resuscitation for hypovolemic shock. Surg. Clin. North Am. 2017, 97, 1307–1321. doi: 10.1016/j. suc.2017.07.011.
- 9. Santry H.P., Alam H.B. Fluid resuscitation: past, present, and the future. Shock. 2010; 33(3): 229–41. doi: 10.1097/SHK.0b013e3181c30f0c.
- 10. Aoki, M., Abe, T., Saitoh, D., Hagiwara, S., Oshima, K. Use of vasopressor increases the risk of mortality in traumatic hemorrhagic shock: a nationwide cohort study in Japan. Crit Care Med 2018, 46(12): e1145-e51.
- 11. Gulati A., Lavhale M., Giri R., Andurkar S., Xanthos T. Centhaquine citrate. Alpha2BAdrenoceptor ligand, resuscitative agent for hypovolemic shock. Drugs Fut. 2020; 45(3): 153–163.
- 12. Szopinski, J., Kusza, K., Semionow, M. Microcirculatory responses to hypovolemic shock. J Trauma 2011, 71(6): 1779-88.
- 13. Gulati A. Vascular endothelium and hypovolemic shock. Curr Vasc Pharmacol. 2016; 14(2): 187–95.
- 14. Kobayashi L., Costantini T.W., Coimbra R. Hypovolemic shock resuscitation. Surg Clin North Am. 2012; 92(6): 1403–23.
- 15. Ranjan A.K., Gulati A. Controls of Central and Peripheral Blood Pressure and Hemorrhagic/ Hypovolemic Shock. Journal of Clinical Medicine. 2023; 12(3): 1108. https://doi.org/10.3390/ jcm12031108.
- 16. Reid J.L. (1986). Alpha-adrenergic receptors and blood pressure control. Am. J. Cardiol. 57, 6E–12E. 10.1016/0002-9149(86)90716-2.
- 17. Bonanno F.G. (2011). Clinical pathology of the shock syndromes. J. Emerg. Trauma Shock 4, 233–243. 10.4103/0974-2700.82211.
- 18. Yoo B., Lemaire A., Mangmool S., Wolf M.J., Curcio A., Mao L., et al. (2009). Beta1-adrenergic receptors stimulate cardiac contractility and CaMKII activation in vivo and enhance cardiac dysfunction following myocardial infarction. Am. J. Physiol. Heart Circ. Physiol. 297, H1377– H1386. 10.1152/ajpheart.00504.2009.
- 19. de Lucia C., Eguchi A., Koch W.J. (2018). New insights in cardiac beta-adrenergic signaling during heart failure and aging. Front. Pharmacol. 9, 904. 10.3389/fphar.2018.00904.
- 20. Xiang L., Hinojosa-Laborde C., Ryan K.L., Rickards C.A., Convertino V.A. Time course of compensatory physiological responses to central hypovolemia in high- and low-tolerant human subjects. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2018; 315: R408–R416. doi: 10.1152/ajpregu.00361.2017.
- 21. Bakker J., Nijsten M.W.N., Jansen T.C. Clinical use of lactate monitoring in critically ill patients. Ann. Intensive Care. 2013;3:12. doi: 10.1186/2110-5820-3-12.
- 22. Standl T., Annecke T., Cascorbi I., Heller A.R., Sabashnikov A., Teske W. The Nomenclature, Denition and Distinction ofTypes of Shock. Dtsch. Arztebl. Int. 2018; 115: 757–768. doi: 10.3238/arztebl.2018.0757.
- 23. Centhaquine: A new resuscitative agent for haemorrhagic shock. 2021 https:// researchoutreach.org/articles/centhaquinenew-resuscitative-agent-haemorrhagic-shock/ Accessed on 1 Oct 2024.
- 24. Lewis S.R., Pritchard M.W., Evans D.J., Butler A.R., Alderson P., Smith A.F., Roberts I. Colloids versus crystalloids for uid resuscitation in critically ill people. Cochrane Database Syst Rev. 2018 Aug 3;8(8):CD000567. doi: 10.1002/14651858.CD000567.
- 25. Vincenzi, R., Cepeda, L.A., Pirani, W.M., Sannomyia, P., Rocha, E.S.M., Cruz, R.J., Jr. Small volume resuscitation with 3% hypertonic saline solution decrease inammatory response and attenuates end organ damage after controlled hemorrhagic shock. Am J Surg 2009, 198(3): 407-14.
- 26. Holcomb J.B., Jenkins D., Rhee P., Johannigman J., Mahoney P., Mehta S., et al. Damage control resuscitation: directly addressing the early coagulopathy of trauma. J Trauma. 2007; 62(2): 307–10.
- 27. Nederpelt C.J., El Hechi M.W., Kongkaewpaisan N., Kokoroskos N, Mendoza A.E, Saillant NN, et al. Fresh frozen plasma-to-packed red blood cell ratio and mortality in traumatic hemorrhage: nationwide analysis of 4,427 patients. J Am Coll Surg. 2020;230(6):893–901.
- 28. Havel, C., Arrich, J., Losert, H., Gamper, G., Mullner, M., Herkner, H. Vasopressors for hypotensive shock. Cochrane Database Syst Rev 2011(5): CD003709.
- 29. Al-Hesayen, A., Parker, J.D. The effects of dobutamine on renal sympathetic activity in human heart failure. J Cardiovasc Pharmacol 2008, 51(5): 434-6.
- 30. Balogh, Z.J., Varga, E., Tomka, J., Suveges, G., Toth, L., Simonka, J.A. The new injury severity score is a better predictor of extended hospitalization and intensive care unit admission than the injury severity score in patients with multiple orthopaedic injuries. J Orthop Trauma 2003, 17(7): 508-12.
- 31. Smart L., Hughes D. The Effects of Resuscitative Fluid Therapy on the Endothelial Surface Layer. Front. Vet. Sci. 2021;8:661660. doi: 10.3389/fvets.2021.661660.
- 32. Ho, A.M., Karmakar, M.K., Contardi, L.H., Ng, S.S., Hewson, J.R. Excessive use of normal saline in managing traumatized patients in shock: a preventable contributor to acidosis. J Trauma 2001, 51(1): 173-7.
- 33. Malone, D.L., Hess, J.R., Fingerhut, A. Massive transfusion practices around the globe and a suggestion for a common massive transfusion protocol. J Trauma 2006, 60(6 Suppl): S91-6.
- 34. Fage, N.; Asfar, P.; Radermacher, P.; Demiselle, J. Norepinephrine and Vasopressin in Hemorrhagic Shock: A Focus on Renal Hemodynamics. Int. J. Mol. Sci. 2023, 24, 4103.
- 35. Abid, O., Akca, S., Haji-Michael, P., Vincent, J.L. Strong vasopressor support may be futile in the intensive care unit patient with multiple organ failure. Crit Care Med 2000, 28(4): 947-9.
- 36. Chalkias A, Koutsovasilis A, Laou E, Papalois A, Xanthos T. Measurement of mean systemic lling pressure after severe hemorrhagic shock in swine anesthetized with propofol-based total intravenous anesthesia: implications for vasopressor-free resuscitation. Acute Crit Care. 2020;35(2):93–101.
- 37. Shen T, Baker K. Venous return and clinical hemodynamics: how the body works during acute hemorrhage. Adv Physiol Educ. 2015;39(4):267–71.
- 38. Alexander, R.S. Venomotor tone in hemorrhage and shock. Circ. Res. 1955, 3, 181–190.
- 39. Chruscinski A., Brede M. E., Meinel L., Lohse M. J., Kobilka B. K., Hein L. (2001)Differential distribution of-adrenergic receptor subtypes in blood vessels of knockout mice lacking 1-or 2-adrenergic receptors. Mol Pharmacol 60 (5), 955–962. 10.1124/mol.60.5.955.
- 40. Philipp M., Brede M., Hein L. (2002). Physiological signicance of alpha(2)- adrenergic receptor subtype diversity: One receptor is not enough. Am. J. Physiol. Regul. Integr. Comp. Physiol. 283, R287–R295. 10.1152/ ajpregu.00123.2002.
- 41. Schwinn D. A., Roehrborn C. G. (2008). Alpha1-adrenoceptor subtypes and lower urinary tract symptoms. Int. J. Urol. 15, 193– 199. 10.1111/j.1442-2042.2007.01956.x.
- 42. Gulati A, Lavhale MS, Garcia DJ, Havalad S. Centhaquin improves resuscitative effect of hypertonic saline in hemorrhaged rats. J Surg Res. 2012;178(1):415–23.
- 43. Gulati A, Hussain G, Srimal RC. Effect of repeated administration of centhaquin, a centrally acting hypotensive drug, on adrenergic, cholinergic (Muscarinic), dopaminergic, and serotonergic receptors in brain-regions of rat. Drug Dev Res. 1991;23(4):307–23.
- 44. Bhalla S., Ali I., Andurkar S. V., Gulati A. (2013). Centhaquin antinociception in mice is mediated by 2A- and 2B- but not 2Cadrenoceptors. Eur. J. Pharmacol. 715, 328–336. 10.1016/j.ejphar.2013.05.004.
- 45. Bhatnagar M, Pande M, Dubey MP, et al. Effect of centhaquine on spontaneous and evoked norepinephrine release from isolated perfused rabbit heart. Arzneimittelforschung 1985;35:693.
- 46. Gulati, A., Zhang, Z., Arshad, K. Centhaquin decreases the requirement of norepinephrine, maintains blood pressure and improves survival following resuscitation of hemorrhaged rats. Crit Care Med 2011, 39(12): 114 (Abst 414). DOI: 10.1097/01.ccm.0000408627.24229.88.
- 47. Bakker J., Coffernils M., Leon M., Gris P., Vincent J. L. (1991). Blood lactate levels are superior to oxygen-derived variables in predicting outcome in human septic shock. Chest 99, 956–962. 10.1378/chest.99.4.956.
- 48. Gulati, A., Zhang, Z., Murphy, A., Lavhale, M.S. Efcacy of centhaquin as a small volume resuscitative agent in severely hemorrhaged rats. Am J Emerg Med 2013, 31(9): 1315-21.
- 49. Gulati, A., Mulloy, N., Zhang, Z., Pais, G. Resuscitative efcacy of centhaquin in a rabbit model of uncontrolled hemorrhagic shock. Crit Care Med 2013, 41(12): Abst 534.
- 50. Papapanagiotou, P., Xanthos, T., Gulati, A. et al. Centhaquin improves survival in a swine model of hemorrhagic shock. J Surg Res 2016, 200(1): 227-35.
- 51. Chalkias A, Pais G, Gulati A. Effect of Centhaquine on the Coagulation Cascade in Normal State and Uncontrolled Hemorrhage: A Multiphase Study Combining Ex Vivo and In Vivo Experiments in Different Species. Int J Mol Sci. 2024 Mar 20;25(6):3494. doi: 10.3390/ ijms25063494.
- 52. Pais, G., Gulati, A. Effect of centhaquin on the coagulation cascade using thromboelastography (Teg). Crit Care Med 2012, 40(12): U56-U7 (Abst 181).
- 53. Harrois A., Soyer B., Gauss T., Hamada S., Raux M., Duranteau J., Langeron O., PaugamBurtz C., Pirracchio R., Riou B., et al. Prevalence and risk factors for acute kidney injury among trauma patients: A multicenter cohort study. Crit. Care. 2018;22:344. doi: 10.1186/s13054- 018-2265-9.
- 54. Legrand M., Mik E.G., Balestra G.M., Lutter R., Pirracchio R., Payen D., Ince C. Fluid resuscitation does not improve renal oxygenation during hemorrhagic shock in rats. Anesthesiology. 2010;112:119–127. doi: 10.1097/ ALN.0b013e3181c4a5e2.
- 55. Basile D.P., Anderson M.D., Sutton T.A. Pathophysiology of acute kidney injury. Compr. Physiol. 2012; 2: 1303–1353. doi: 10.1002/cphy. c110041.
- 56. Ranjan, A., Briyal, S., Zhang, Z., Marwah, M., Posen, M., Cherian, V., et al. (2020). Centhaquine upregulates hif1-a and protects hemorrhage-induced acute kidney injury. Crit. Care Med. 48, 690. doi:10.1097/01. ccm.0000645620.40050.9f.
- 57. Ranjan, A. K., Zhang, Z., Briyal, S., and Gulati, A.(2021).Centhaquinerestoresrenalbloodow and protects tissue damage after hemorrhagic shock and renal ischemia. Front. Pharmacol. 12, 616253. doi:10.3389/fphar.2021.616253.
- 58. Jackson C.A., Insel P.A. (1993). Renal ?-adrenergic receptors and genetic hypertension. Pediatr. Nephrol. 7, 853–858. 10.1007/bf01213373.
- 59. de Leeuw P. W., Birkenhager W. H. (1988). Alpha-adrenoceptors and the kidney. J. Hypertens. 6, S21–S24. 10.1097/00004872- 198812001-00004.
- 60. Gulati A. J., Dinesh, Agrawal Nilesh., Rahate Prashant., Das Soumen., Chowdhuri Rajat., et al. (2019).Clinical phase II results OF PMZ2010 (centhaquin) as a resuscitative agent for hypovolemic SHOCK. Crit. Care Med. 47, 1. 10.1097/01.ccm.0000550815.69306.46.
- 61. Gulati A, Jain D, Agrawal NR, Rahate P, Choudhuri R, Das S, Dhibar DP, Prabhu M, Haveri S, Agarwal R, Lavhale MS. Resuscitative Effect of Centhaquine (Lyfaquin®) in Hypovolemic Shock Patients: A Randomized, Multicentric, Controlled Trial. Adv Ther. 2021 Jun;38(6):3223-3265. doi: 10.1007/s12325-021- 01760-4.
- 62. Kumar, A.; Anel, R.; Bunnell, E.; Zanotti, S.; Habet, K.; Haery, C.; Marshall, S.; Cheang, M.; Neumann, A.; Ali, A.; et al. Preloadindependent mechanisms contribute to increased stroke volume following large volume saline infusion in normal volunteers: A prospective interventional study. Crit. Care 2004, 8, R128–R136.
- 63. Centhaquine: New Hope! Amanpreet Singh Wasir, chitra mehta, Yatin Mehta, Dr.Bhawna Sharma. JACC April 2, 2024 Volume 83, Issue 13, Suppl A.
- 64. Lifaquin Prescribing Information, July 2020.
- 65. Huette, P., Moussa, M.D., Beyls, C. et al. Association between acute kidney injury and norepinephrine use following cardiac surgery: a retrospective propensity score-weighted analysis. Ann. Intensive Care 12, 61 (2022). https://doi.org/10.1186/s13613-022-01037-1.
- 66. Giancarelli A, Birrer KL, Alban RF, Hobbs BP, Liu-DeRyke X. Hypocalcemia in trauma patients receiving massive transfusion. J Surg Res. 2016;202(1):182–7.
- 67. Ditzel RM Jr, Anderson JL, Eisenhart WJ, Rankin CJ, DeFeo DR, Oak S, et al. A review of transfusion- and trauma-induced hypocalcemia: Is it time to change the lethal triad to the lethal diamond? J Trauma Acute Care Surg. 2020;88(3):434–9.
Data Sharing Statement
There are no additional data available.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
Information not provided.
Conflicts of Interest
The author report no conflicts of interest in this work.
About this article
Cite this article
Shah S. Bridging the gap in resuscitation therapies: centhaquine in hypovolemic shock. Ind J Emerg Med. 2025;11(1):13-25.
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| January 11, 2025 | February 14, 2025 | April 20, 2025 |
DOI: https://doi.org/10.21088/ijem.2395.311X.11125.2
Keywords
CenthaquineHypovolemic shockResuscitation therapyHemodynamic stabilityOrgan protectionTissue perfusionMultiorgan failureSearch for Similar Articles
Similar Articles
- Covid 19 Vaccine: Associated Henoch Schonlein Purpura in Young Adult Female
- A Rare Case of Intolerance to Medically Approved Dose of Sildenafil Citrate in a...
- Acute Mesenteric Ischemia: An Unusual Cause of Hematemesis in a 48 Year Old Man
- Brachial Artery Pseudoaneurysm Related Causally to Iatrogenic Coagulopathy in a...
- Combination Therapy for Acute Management of Yellow Oleander Poisoning: A Case Re...
Article Level Metrics
Last UpdatedTuesday 07 July 2026, 12:38:54 (IST)
2530
Accesses
15
890
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | January 11, 2025 |
| Accepted | February 14, 2025 |
| Published | April 20, 2025 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.