Full Text (PDF)
Urology, Nephrology and Andrology International 10(1):p 27-30, Jan -June 2025. | DOI: 10.21088/unai.2456-5016.10125.4
Case Report
Renal Hydatid Cyst: Diagnostic Insights from Imaging
Prabh Simranpal, Ashishjot Kaur, Rishab Garg
Author Information
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
Urology, Nephrology and Andrology International 10(1):p 27-30, Jan -June 2025. | DOI: 10.21088/unai.2456-5016.10125.4
How Cite This Article:
Timeline
Received : October 11, 2025
Accepted : November 07, 2025
Published : November 14, 2025
Abstract
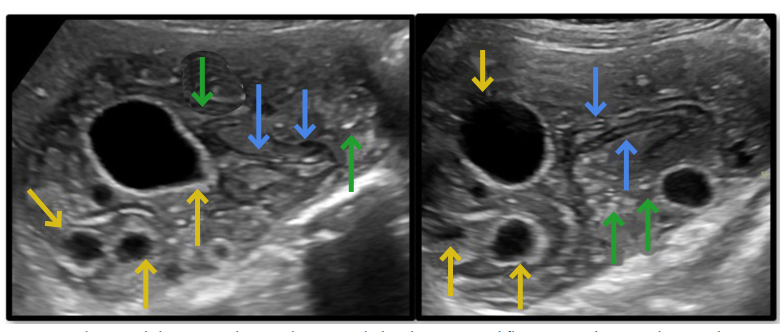
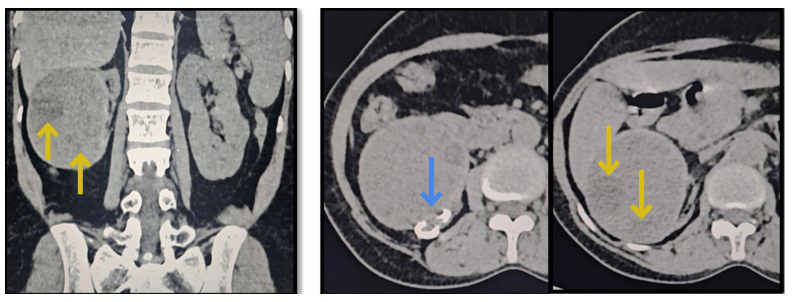
Renal hydatid cyst is an uncommon manifestation of cystic echinococcosis and often poses a diagnostic challenge due to non-specific clinical presentation. Imaging techniques, particularly ultrasonography (US) and computed tomography (CT), are pivotal for early and accurate diagnosis, while serology may be inconclusive. Surgical removal combined with anti-helminthic therapy remains the cornerstone of management. We report a case of solitary renal hydatid cyst in a 45-year-old woman, describe characteristic imaging features, and review diagnostic and therapeutic strategies.
References
- 1. Polat P., Kantarci M., Alper F., Suma S., Koruyucu M.B., Okur A. Hydatid disease from head to toe. Radiographics. 2003; 23(2): 475–94. doi:10.1148/rg.232025704.
- 2. Brunetti E., Kern P., Vuitton D.A.; Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010; 114(1): 1–16. doi:10.1016/j. actatropica.2009.11.001.
- 3. Mohammed S.A., Molla M.G., Bekele F.S., Endris H.S. Isolated renal hydatid cyst. Int J Surg Case Rep. 2023; 109: 109167. doi:10.1016/j. ijscr.2023.109167.
- 4. Junghanss T., Menezes da Silva A., Horton J., Chiodini P.L., Brunetti E. Clinical management of cystic echinococcosis: state of the art, problems, and perspectives. Clin Microbiol Rev. 2008; 21(2): 289–318.
- 5. Ramteke V.V., Deshpande N.S., Balwani MR, Bawankule C.P. Primary renal echinococcosis. Indian J Nephrol. (provide year and volume if required). doi:10.4103/0971-4065.202839. Ashishjot Kaur, Prabh Simranpal, Rishab Garg. Renal Hydatid Cyst: Diagnostic Insights from Imaging.30 Urology, Nephrology and Andrology International UNAI / Volume 10 Number 1 / January-June 2025
- 6. Sharma K., Sharma R., Tiwari T., et al. Primary renal hydatid cyst. BMJ Case Rep. 2022;15:e248006. doi:10.1136/bcr-2021-248006
- 7. Romig T., Zeyhle E., Macpherson C.N., Rees P.H., Were J.B. Cyst growth and spontaneous cure in hydatid disease. Lancet. 1986; 1: 861.
- 8. Brunetti E., Troìa G., Gulizia R., Garlaschelli AL, Filice C. ‘Watch and Wait’ as an alternative treatment for active and transitional echinococcal cysts: single-center experience. Am J Trop Med Hyg. 2005; 73(1): 29–32.
- 9. Polat P., Kantarci M., Alper F., et al. Hydatid disease from head to toe. Radiographics 2003; 23: 475–94.
Data Sharing Statement
There are no additional data available. All raw data and code are available upon request.
Funding
This research received no funding.
Author Contributions
All authors contributed significantly to the work and approve its publication.
Ethics Declaration
This article does not involve any human or animal subjects, and therefore does not require ethics approval.
Acknowledgements
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
Conflicts of Interest
No conflicts of interest.
About this article
Cite this article
Licence:
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.
| Received | Accepted | Published |
|---|---|---|
| October 11, 2025 | November 07, 2025 | November 14, 2025 |
DOI: 10.21088/unai.2456-5016.10125.4
Keywords
Renal hydatid cystEchinococcosisUltrasoundComputed tomographySearch for Similar Articles
Similar Articles
- Skin and Nail Hyperpigmentation (Melanonychia) Due to Cyclophosphamide in Steroi...
- Rirs: A Modality of Choice for Stone Clearance in Abnormally Fused Ectopic Kidne...
- Environmental Nephrology: A Comprehensive Narrative Review
- Bilateral Testicular Germ Cell Tumor: A Rare Entity
- The Effectiveness of Alarm Therapy in Treating Nocturnal Enuresis in Children:...
Article Level Metrics
Last UpdatedWednesday 17 June 2026, 19:05:31 (IST)
348
Accesses
6
76
00
Citations
NA
NA
NA
Download citation
Article Keywords
Keyword Highlighting
Highlight selected keywords in the article text.
Timeline
| Received | October 11, 2025 |
| Accepted | November 07, 2025 |
| Published | November 14, 2025 |
licence
Attribution-Non-commercial 4.0 International (CC BY-NC 4.0)
This license enables reusers to distribute, remix, adapt, and build upon the material in any medium or format for noncommercial purposes only, and only so long as attribution is given to the creator.